

Pediatric sensorineural hearing loss, part 2: syndromic and acquired causes
- PMID: 21596810
- PMCID: PMC7966448
- DOI: 10.3174/ajnr.A2499
Pediatric sensorineural hearing loss, part 2: syndromic and acquired causes
Abstract
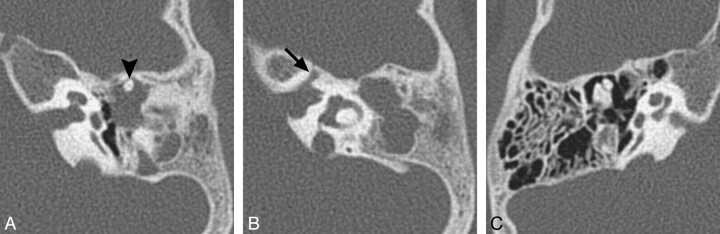
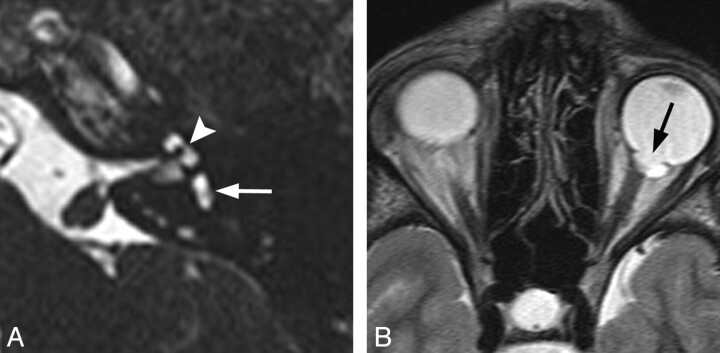
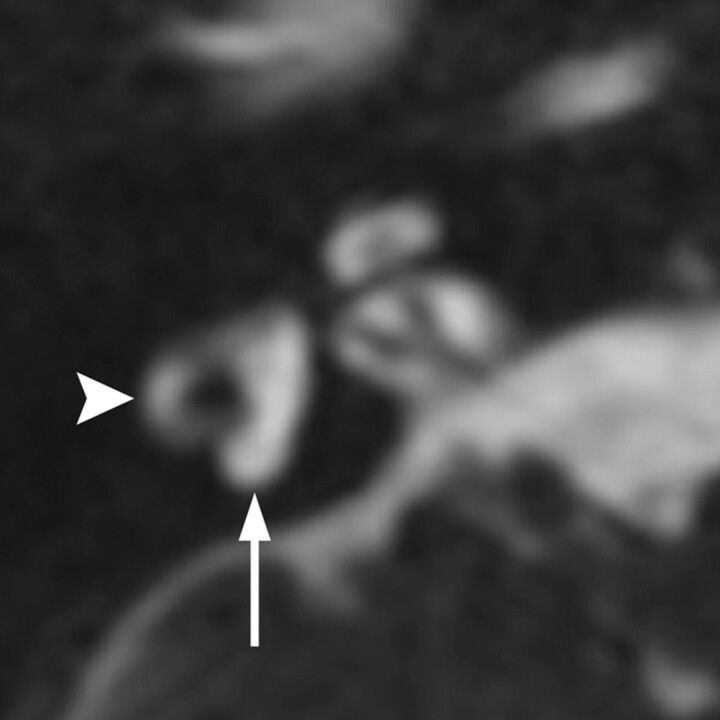
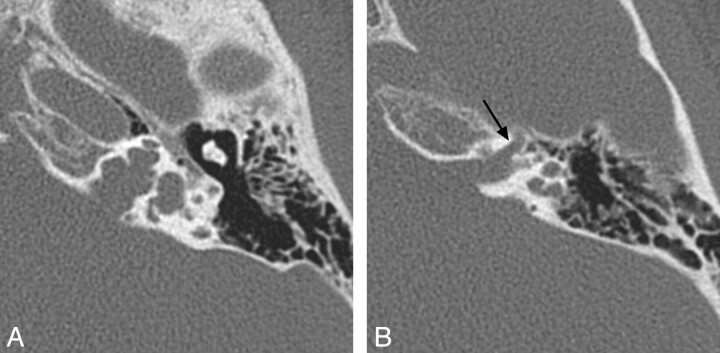
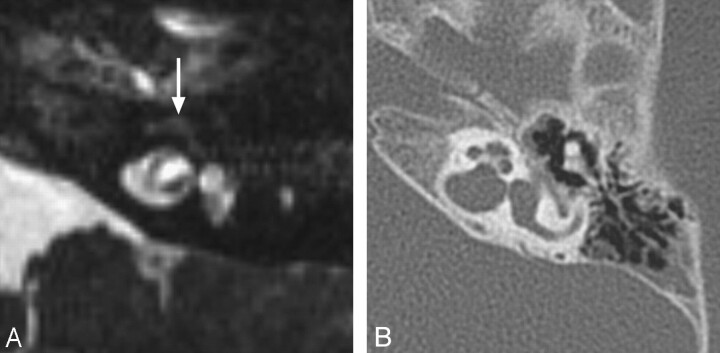
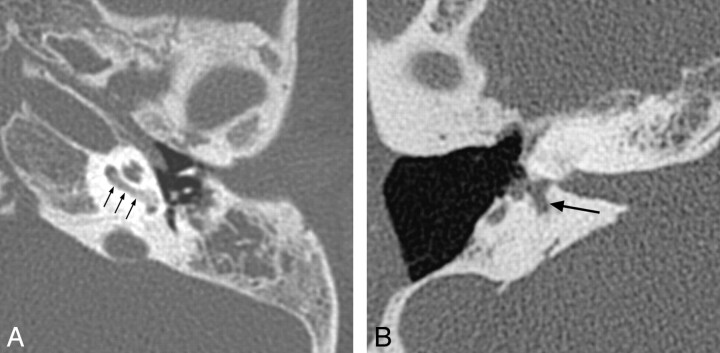
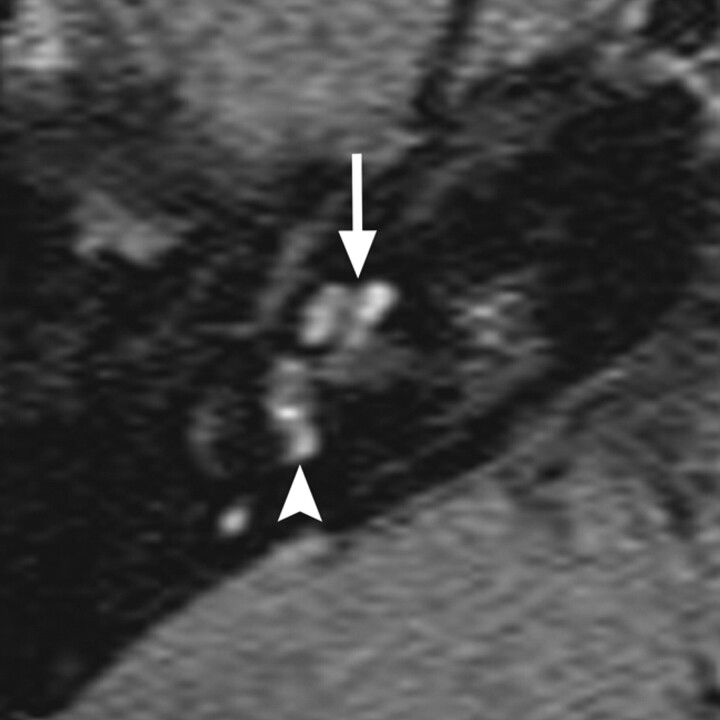
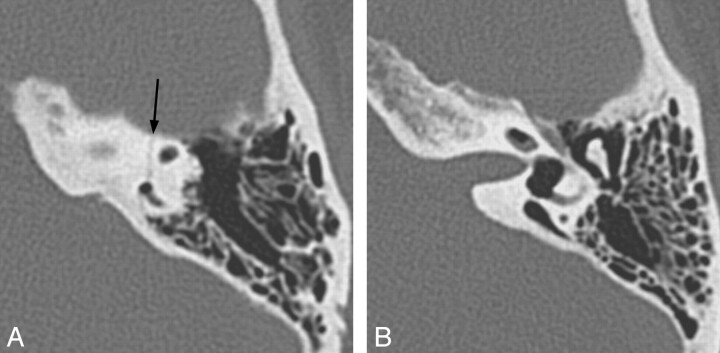
This article is the second in a 2-part series reviewing neuroimaging in childhood SNHL. Previously, we discussed the clinical work-up of children with hearing impairment, the classification of inner ear malformations, and congenital nonsyndromic causes of hearing loss. Here, we review and illustrate the most common syndromic hereditary and acquired causes of childhood SNHL, with an emphasis on entities that demonstrate inner ear abnormalities on cross-sectional imaging. Syndromes discussed include BOR syndrome, CHARGE syndrome, Pendred syndrome, Waardenburg syndrome, and X-linked hearing loss with stapes gusher. We conclude the article with a review of acquired causes of childhood SNHL, including infections, trauma, and neoplasms.
Figures
References
-
- Billings KR, Kenna MA. Causes of pediatric sensorineural hearing loss: yesterday and today. Arch Otolaryngol Head Neck Surg 1999; 125: 517– 21 - PubMed
-
- Lalwani AK, Castelein CM. Cracking the auditory genetic code: nonsyndromic hereditary hearing impairment. Am J Otol Jan 1999; 20: 115– 32 - PubMed
-
- Morton CC, Nance WE. Newborn hearing screening: a silent revolution. N Engl J Med 2006; 354: 2151– 64 - PubMed
-
- Kochhar A, Fischer SM, Kimberling WJ, et al. Branchio-oto-renal syndrome. Am J Med Genet A 2007; 143A: 1671– 78 - PubMed
-
- Propst EJ, Blaser S, Gordon KA, et al. Temporal bone findings on computed tomography imaging in branchio-oto-renal syndrome. Laryngoscope 2005; 115: 1855– 62 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials