

Frequent hemodialysis schedules are associated with reduced levels of dialysis-induced cardiac injury (myocardial stunning)
- PMID: 21597028
- PMCID: PMC3109928
- DOI: 10.2215/CJN.05200610
Frequent hemodialysis schedules are associated with reduced levels of dialysis-induced cardiac injury (myocardial stunning)
Abstract
Background and objectives: Recurrent hemodialysis (HD)-induced ischemic cardiac injury (myocardial stunning) is common and associated with high ultrafiltration (UF) requirements, intradialytic hypotension, long-term loss of systolic function, increased likelihood of cardiovascular events, and death. More frequent HD regimens are associated with lower UF requirements and improved hemodynamic tolerability, improved cardiovascular outcomes, and reduced mortality compared with conventional thrice-weekly HD. This study investigated the hypothesis that modification of UF volume and rate with more frequent HD therapies would abrogate dialysis-induced myocardial stunning.
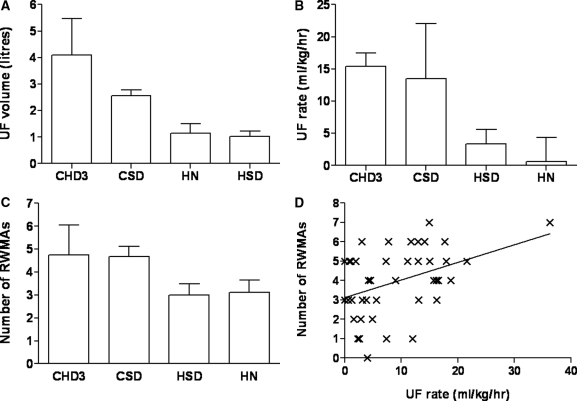
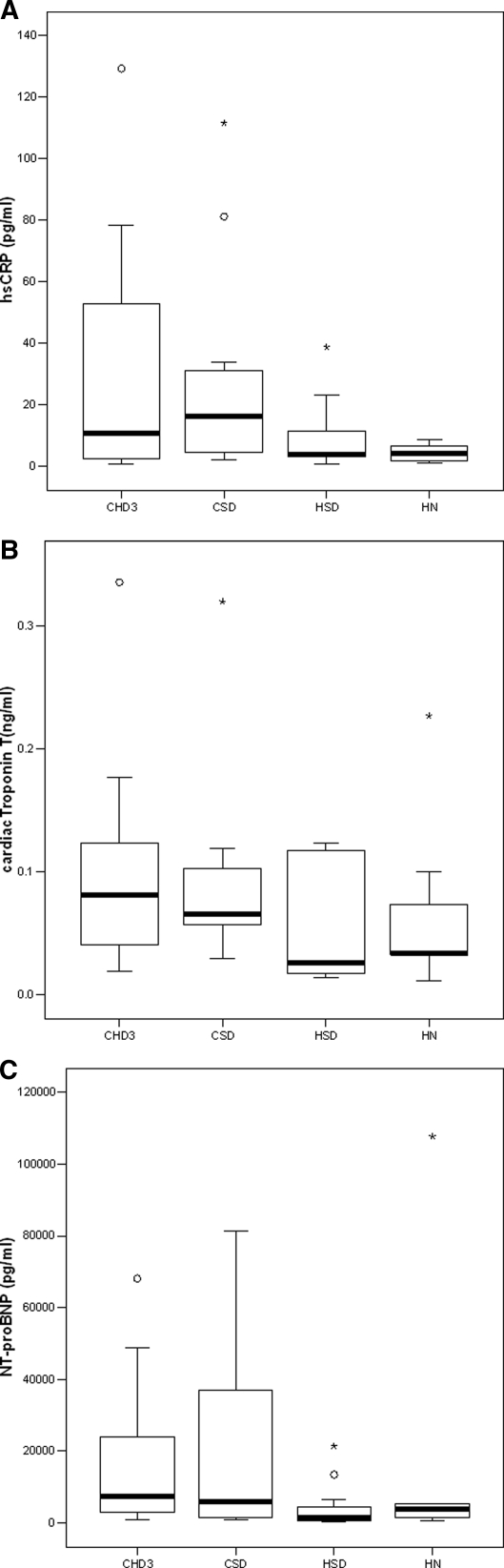
Design, settings, participants, & measurements: A cross-sectional study of 46 patients established on hemodialysis >3 months compared four groups receiving the current range of quotidian therapies: conventional thrice-weekly HD (CHD3); more-frequent HD five to six times/week in a center (CSD) and at home (HSD); and home nocturnal HD (HN). Serial echocardiography quantitatively assessed regional systolic function to identify intradialytic left ventricular regional wall motion abnormalities (RWMAs). Cardiac troponin T (cTnT), N-terminal prohormone brain natriuretic peptide (NT-proBNP), and inflammatory markers were quantified.
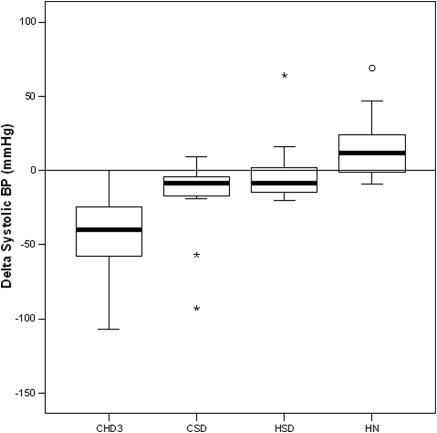
Results: More frequent HD regimens were associated with lower UF volumes and rates compared with CHD3. Intradialytic fall in systolic BP was reduced in CSD and HSD groups and abolished in HN group. Mean RWMAs per patient reduced with increasing dialysis intensity (CHD3 > CSD > HSD > HN). Home-based groups demonstrated lower high-sensitivity C-reative protein levels, with trends to lower cTnT and NT-proBNP levels in the more frequent groups.
Conclusions: Frequent HD regimes are associated with less dialysis-induced myocardial stunning compared with conventional HD. This may contribute to improved outcomes associated with frequent HD therapies.
Figures
Comment in
-
Is hemodialysis bad for the heart?Semin Dial. 2012 Jan-Feb;25(1):86-7. doi: 10.1111/j.1525-139X.2011.01043.x. Semin Dial. 2012. PMID: 22273531 No abstract available.
References
-
- Foley RN, Parfrey PS: Cardiovascular disease and mortality in ESRD. J Nephrol 11: 239–245, 1998 - PubMed
-
- Sigrist MK, Taal MW, Bungay P, McIntyre CW: Progressive vascular calcification over 2 years is associated with arterial stiffening and increased mortality in patients with stages 4 and 5 chronic kidney disease. Clin J Am Soc Nephrol 2: 1241–1248, 2007 - PubMed
-
- Ichimaru K, Horie A: Microangiopathic changes of subepidermal capillaries in end-stage renal failure. Nephron 46: 144–149, 1987 - PubMed
-
- Ragosta M, Samady H, Isaacs RB, Gimple LW, Sarembock IJ, Powers ER: Coronary flow reserve abnormalities in patients with diabetes mellitus who have end-stage renal disease and normal epicardial coronary arteries. Am Heart J 147: 1017–1023, 2004 - PubMed
-
- Selby NM, Burton JO, Chesterton LJ, McIntyre CW: Dialysis-induced regional left ventricular dysfunction is ameliorated by cooling the dialysate. Clin J Am Soc Nephrol 1: 1216–1225, 2006 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
