

Clinical, quality of life, and economic value of acromegaly disease control
- PMID: 21597975
- PMCID: PMC3146976
- DOI: 10.1007/s11102-011-0310-7
Clinical, quality of life, and economic value of acromegaly disease control
Abstract
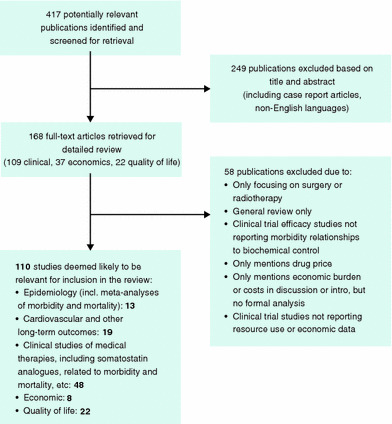
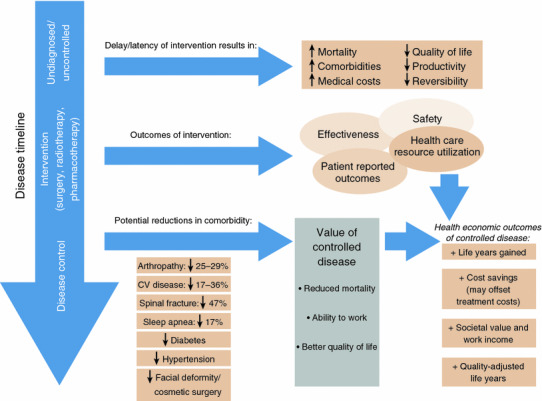
Although acromegaly is a rare disease, the clinical, economic and health-related quality of life (HRQoL) burden is considerable due to the broad spectrum of comorbidities as well as the need for lifelong management. We performed a comprehensive literature review of the past 12 years (1998-2010) to determine the benefit of disease control (defined as a growth hormone [GH] concentration <2.5 μg/l and insulin-like growth factor [IGF]-1 normal for age) on clinical, HRQoL, and economic outcomes. Increased GH and IGF-1 levels and low frequency of somatostatin analogue use directly predicted increased mortality risk. Clinical outcome measures that may improve with disease control include joint articular cartilage thickness, vertebral fractures, left ventricular function, exercise capacity and endurance, lipid profile, and obstructive apnea events. Some evidence suggests an association between controlled disease and improved HRQoL. Total direct treatment costs were higher for patients with uncontrolled compared to controlled disease. Costs incurred for management of comorbidities, and indirect cost could further add to treatment costs. Optimizing disease control in patients with acromegaly appears to improve outcomes. Future studies need to evaluate clinical outcomes, as well as HRQoL and comprehensive economic outcomes achieved with controlled disease.
Conflict of interest statement
This research was funded by Novartis Pharmaceuticals.
Figures


References
-
- Drange MR, Fram NR, Herman-Bonert V, Melmed S (2000) Pituitary tumor registry: a novel clinical resource. J Clin Endocrinol Metab 85:168–174 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
