

Early infant HIV-1 diagnosis programs in resource-limited settings: opportunities for improved outcomes and more cost-effective interventions
- PMID: 21599888
- PMCID: PMC3129310
- DOI: 10.1186/1741-7015-9-59
Early infant HIV-1 diagnosis programs in resource-limited settings: opportunities for improved outcomes and more cost-effective interventions
Abstract
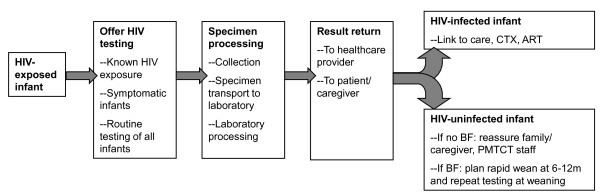
Early infant diagnosis (EID) of HIV-1 infection confers substantial benefits to HIV-infected and HIV-uninfected infants, to their families, and to programs providing prevention of mother-to-child transmission (PMTCT) services, but has been challenging to implement in resource-limited settings. In order to correctly inform parents/caregivers of infant infection status and link HIV-infected infants to care and treatment, a 'cascade' of events must successfully occur. A frequently cited barrier to expansion of EID programs is the cost of the required laboratory assays. However, substantial implementation barriers, as well as personnel and infrastructure requirements, exist at each step in the cascade. In this update, we review challenges to uptake at each step in the EID cascade, highlighting that even with the highest reported levels of uptake, nearly half of HIV-infected infants may not complete the cascade successfully. We next synthesize the available literature about the costs and cost effectiveness of EID programs; identify areas for future research; and place these findings within the context of the benefits and challenges to EID implementation in resource-limited settings.
Figures
References
-
- UNAIDS/UNICEF/WHO. Children and AIDS: Fourth stocktaking report, actions and progress. http://www.unicef.org/publications/index_46585.html
-
- World Health Organization. Towards universal access: Scaling up priority HIV/AIDS interventions in the health sector. Progress Report. http://www.who.int/hiv/pub/2010progressreport/report/en/index.html
-
- Creek T, Tanuri A, Smith M, Seipone K, Smit M, Legwaila K, Motswere C, Maruping M, Nkoane T, Ntumy R, Bile E, Mine M, Lu L, Tebele G, Mazhani L, Davis MK, Roels TH, Kilmarx PH, Shaffer N. Early diagnosis of human immunodeficiency virus in infants using polymerase chain reaction on dried blood spots in Botswana's national program for prevention of mother-to-child transmission. Pediatr Infect Dis J. 2008;27:22–26. doi: 10.1097/INF.0b013e3181469050. - DOI - PubMed
-
- Barker PM, Mphatswe W, Rollins N. Antiretroviral drugs in the cupboard are not enough: the impact of health Systems' performance on mother-to-child transmission of HIV. J Acquir Immune Defic Syndr. 2010;56:e45–48. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
