

Age-specific differences in influenza A epidemic curves: do children drive the spread of influenza epidemics?
- PMID: 21602300
- PMCID: PMC3119537
- DOI: 10.1093/aje/kwr037
Age-specific differences in influenza A epidemic curves: do children drive the spread of influenza epidemics?
Abstract
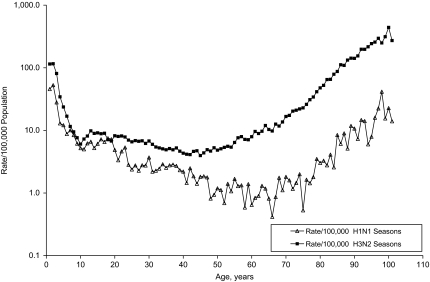
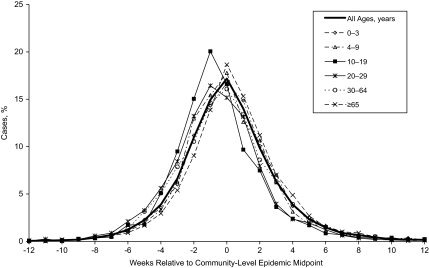
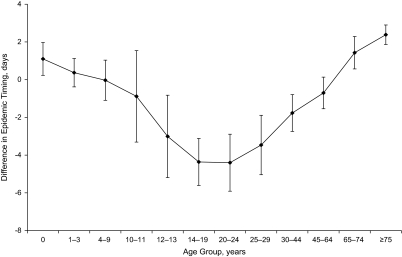
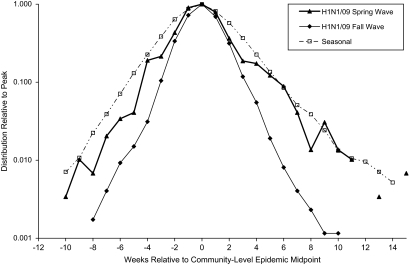
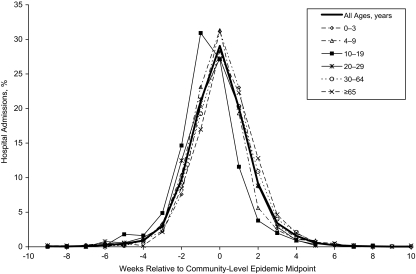
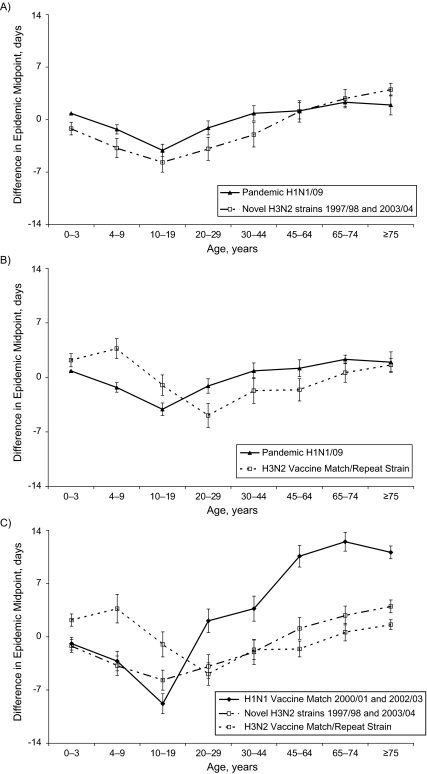
There is accumulating evidence suggesting that children may drive the spread of influenza epidemics. The objective of this study was to quantify the lead time by age using laboratory-confirmed cases of influenza A for the 1995/1996-2005/2006 seasons from Canadian communities and laboratory-confirmed hospital admissions for the H1N1/2009 pandemic strain. With alignment of the epidemic curves locally before aggregation of cases, slight age-specific differences in the timing of infection became apparent. For seasonal influenza, both the 10-19- and 20-29-year age groups peaked 1 week earlier than other age groups, while during the fall wave of the 2009 pandemic, infections peaked earlier among only the 10-19-year age group. In the H3N2 seasons, infections occurred an average of 3.9 (95% confidence interval: 1.7, 6.1) days earlier in the 20-29-year age group than for youth aged 10-19 years, while during the fall pandemic wave, the 10-19-year age group had a statistically significant lead of 3 days compared with both younger children aged 4-9 years and adults aged 20-29 years (P < 0.0001). This analysis casts doubt on the hypothesis that younger school-age children actually lead influenza epidemic waves.
Figures
References
-
- Longini IM, Jr, Koopman JS, Haber M, et al. Statistical inference for infectious diseases. Risk-specific household and community transmission parameters. Am J Epidemiol. 1988;128(4):845–859. - PubMed
-
- Wallinga J, Teunis P, Kretzschmar M. Using data on social contacts to estimate age-specific transmission parameters for respiratory-spread infectious agents. Am J Epidemiol. 2006;164(10):936–944. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
