

A long-term prospective study of type-specific human papillomavirus infection and risk of cervical neoplasia among 20,000 women in the Portland Kaiser Cohort Study
- PMID: 21602310
- PMCID: PMC3156084
- DOI: 10.1158/1055-9965.EPI-11-0206
A long-term prospective study of type-specific human papillomavirus infection and risk of cervical neoplasia among 20,000 women in the Portland Kaiser Cohort Study
Erratum in
- Cancer Epidemiol Biomarkers Prev. 2012 Aug;21(8):1390-1
Abstract
Background: Human papillomavirus (HPV) DNA testing is more sensitive than cytology for detection of cervical intraepithelial neoplasia grade 3 and cancer (≥CIN3). Adding HPV testing to cytology is recommended for women ≥30 but long-term prospective studies of HPV testing are rare.
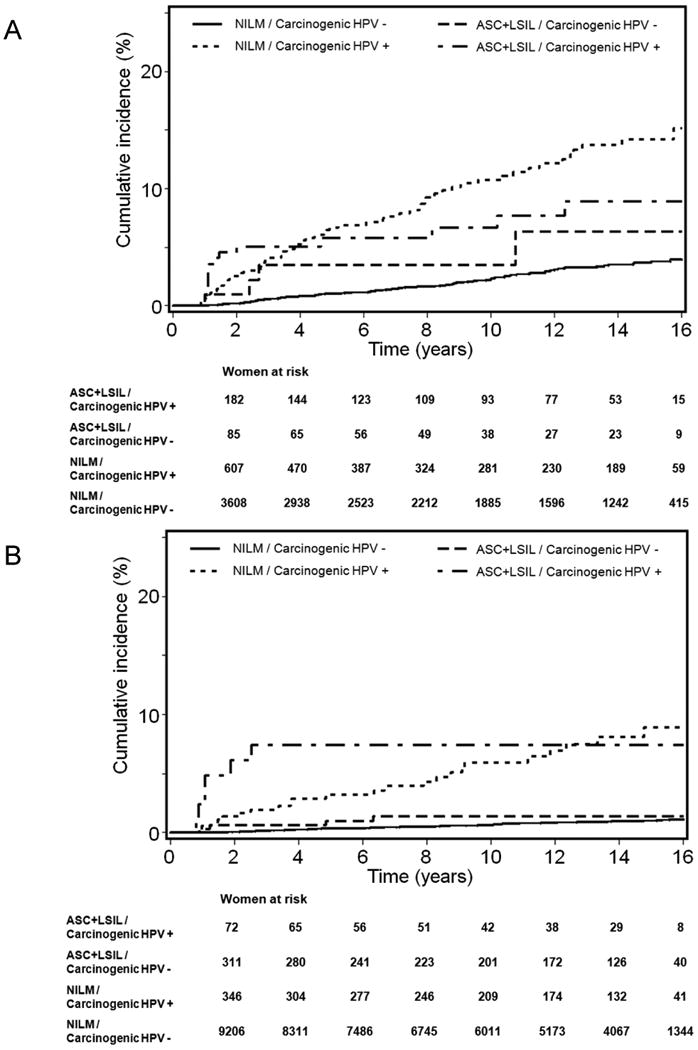
Methods: Beginning in 1989-1990, ~20,000 women in a prepaid health maintenance organization (median age = 34) were followed passively by recommended annual cytology. We tested archived cervicovaginal lavage specimens collected at enrollment, primarily by MY09-MY11 PCR-based methods, for carcinogenic HPV types. We calculated positive and negative predictive values for the entire study period, and Kaplan-Meier estimates of cumulative probability for ≥CIN3, up to 18 years of follow-up.
Results: We observed 47 cases of invasive cervical cancer during the study period, and 156 cases of CIN3. Predictive values and Kaplan-Meier analyses yielded the same conclusions. In women 30 and older, the reassurance against ≥CIN3 following a single negative HPV test was long-lasting (cumulative probability = 0.7% during follow-up). In this age group, a single HPV test (positive vs. negative, hazard ratio of 8.5, 95% CI = 4.8-15.1) provided greater long-term risk stratification than a single cytologic result (abnormal vs. normal, HR = 2.9, 95% CI = 1.2-6.6). The risk for ≥CIN3 was higher for HPV16 than for the average of the other carcinogenic types (hazard ratio = 2.7).
Conclusion and impact: The data from this cohort study show the long-term predictive value of HPV testing, particularly in women ≥30, and a possible role for distinguishing particularly carcinogenic types like HPV16.
©2011 AACR
Figures




References
-
- Bosch FX, Manos MM, Munoz N, et al. Prevalence of human papillomavirus in cervical cancer: a worldwide perspective. International biological study on cervical cancer (IBSCC) Study Group. J Natl Cancer Inst. 1995;87:796–802. - PubMed
-
- Reeves WC, Brinton LA, Garcia M, et al. Human papillomavirus infection and cervical cancer in Latin America. N Engl J Med. 1989;320:1437–41. - PubMed
-
- Sherman ME, Lorincz AT, Scott DR, et al. Baseline cytology, human papillomavirus testing, and risk for cervical neoplasia: a 10-year cohort analysis. J Natl Cancer Inst. 2003;95:46–52. - PubMed
