

Effects of a flexibility and relaxation programme, walking, and nordic walking on Parkinson's disease
- PMID: 21603199
- PMCID: PMC3095265
- DOI: 10.4061/2011/232473
Effects of a flexibility and relaxation programme, walking, and nordic walking on Parkinson's disease
Abstract
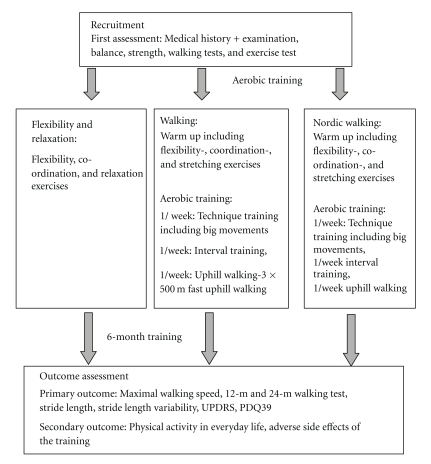
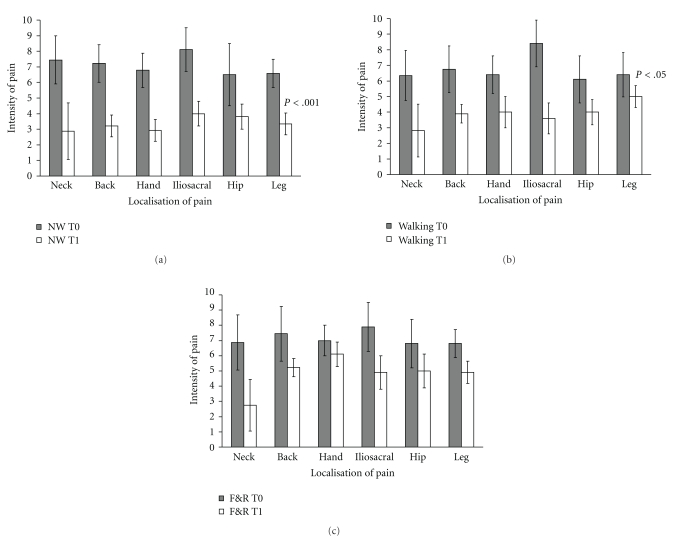
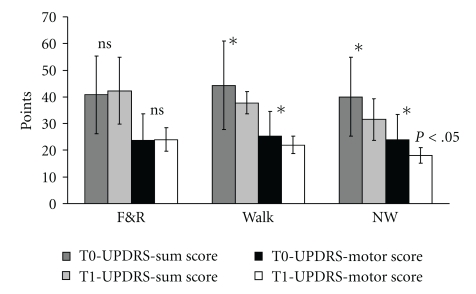
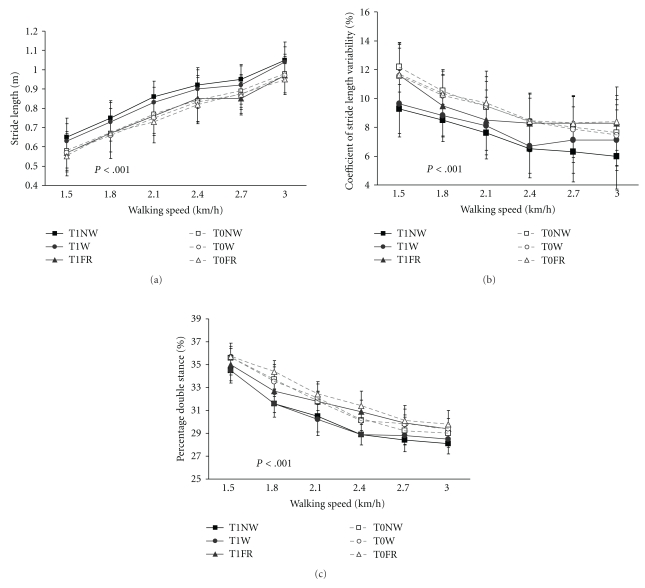
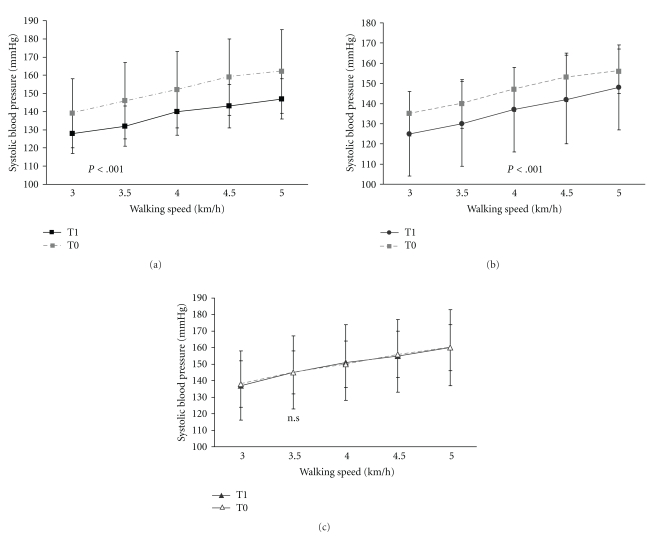
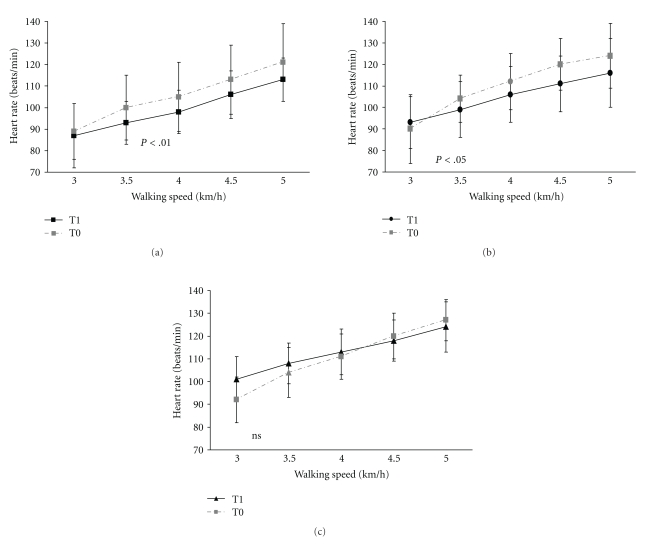
Symptoms of Parkinson's disease (PD) progress despite optimized medical treatment. The present study investigated the effects of a flexibility and relaxation programme, walking, and Nordic walking (NW) on walking speed, stride length, stride length variability, Parkinson-specific disability (UPDRS), and health-related quality of life (PDQ 39). 90 PD patients were randomly allocated to the 3 treatment groups. Patients participated in a 6-month study with 3 exercise sessions per week, each lasting 70 min. Assessment after completion of the training showed that pain was reduced in all groups, and balance and health-related quality of life were improved. Furthermore, walking, and Nordic walking improved stride length, gait variability, maximal walking speed, exercise capacity at submaximal level, and PD disease-specific disability on the UPDRS in addition. Nordic walking was superior to the flexibility and relaxation programme and walking in improving postural stability, stride length, gait pattern and gait variability. No significant injuries occurred during the training. All patients of the Nordic walking group continued Nordic walking after completing the study.
Figures
References
-
- Chen RC, Chang SF, Su CL, et al. Prevalence, incidence, and mortality of PD: a door-to-door survey in Ilan County, Taiwan. Neurology. 2001;57(9):1679–1686. - PubMed
-
- Caradoc-Davies TH, Weatherall M, Dixon GS, Caradoc-Davies G, Hantz P. Is the prevalence of Parkinson’s disease in New Zealand really changing? Acta Neurologica Scandinavica. 1992;86(1):40–44. - PubMed
-
- Gelb DJ, Oliver E, Gilman S. Diagnostic criteria for Parkinson disease. Archives of Neurology. 1999;56(1):33–39. - PubMed
LinkOut - more resources
Full Text Sources
Medical
