

C-Reactive Protein: How Has JUPITER Impacted Clinical Practice?
- PMID: 21603445
- PMCID: PMC3096289
C-Reactive Protein: How Has JUPITER Impacted Clinical Practice?
Abstract
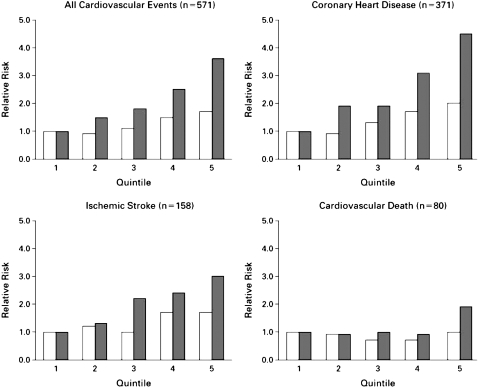
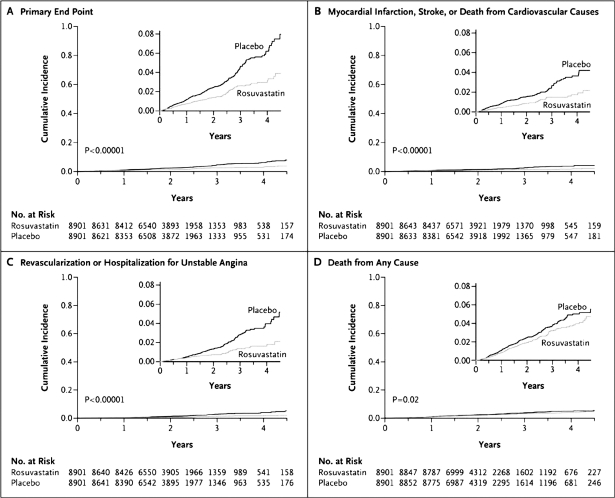
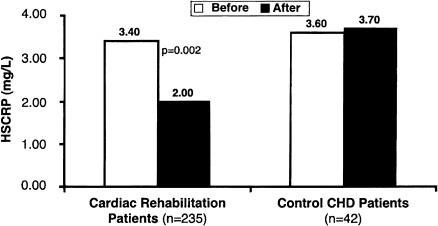
Inflammation plays a pivotal role in all phases of atherosclerosis. High-sensitivity C-reactive protein (hsCRP), the best characterized biomarker of inflammation, is an independent predictor of future cardiovascular (CV) events and can add further insight to risk stratification. Assessment of hsCRP levels in clinical practice is feasible and inexpensive. Justification for the Use of Statins in Primary Prevention: An Intervention Trial Evaluating Rosuvastatin (JUPITER) was a landmark primary prevention trial that enrolled 17,802 apparently healthy men and women with low-density lipoprotein cholesterol levels of less than 130 mg/dL and hsCRP levels of 2 mg/L or higher and randomly assigned them to rosuvastatin, 20 mg daily, or placebo. The trial demonstrated that treatment with statin was associated with significant lowering of hsCRP (37%), with 44% reduction in incident CV and 20% reduction in all-cause mortality. These compelling data from the JUPITER trial should encourage changes in our approach toward primary prevention of CV disease and lipid-lowering therapy, as these data shift the focus toward a link between inflammation, statin therapy, and prevention of atherosclerotic CV diseases.
Keywords: C-reactive protein; Cardiovascular disease; JUPITER; coronary artery disease; risk factor.
Figures
References
-
- Ross R. Atherosclerosis: an inflammatory disease. N Engl J Med. 1999;340:115–126. - PubMed
-
- Libby P., Ridker P. M., Maseri A. Inflammation and atherosclerosis. Circulation. 2002;105:1135–1143. - PubMed
-
- Hansson G. K. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. 2005;352:1685–1695. - PubMed
-
- Burke A. P., Tracy R. P., Kolodgie F., et al. Elevated C-reactive protein values and atherosclerosis in sudden coronary death: association with different pathologies. Circulation. 2002;105:2019–2023. - PubMed
-
- Ridker P. M., Hennekens C. H., Buring J. E., Rifai N. C-reactive protein and other markers of inflammation in the prediction of cardiovascular disease in women. N Engl J Med. 2000;342:836–843. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials