

Diagnosis and treatment of chronic constipation--a European perspective
- PMID: 21605282
- PMCID: PMC3170709
- DOI: 10.1111/j.1365-2982.2011.01709.x
Diagnosis and treatment of chronic constipation--a European perspective
Abstract
Background: Although constipation can be a chronic and severe problem, it is largely treated empirically. Evidence for the efficacy of some of the older laxatives from well-designed trials is limited. Patients often report high levels of dissatisfaction with their treatment, which is attributed to a lack of efficacy or unpleasant side-effects. Management guidelines and recommendations are limited and are not sufficiently current to include treatments that became available more recently, such as prokinetic agents in Europe.
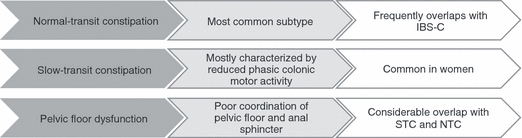
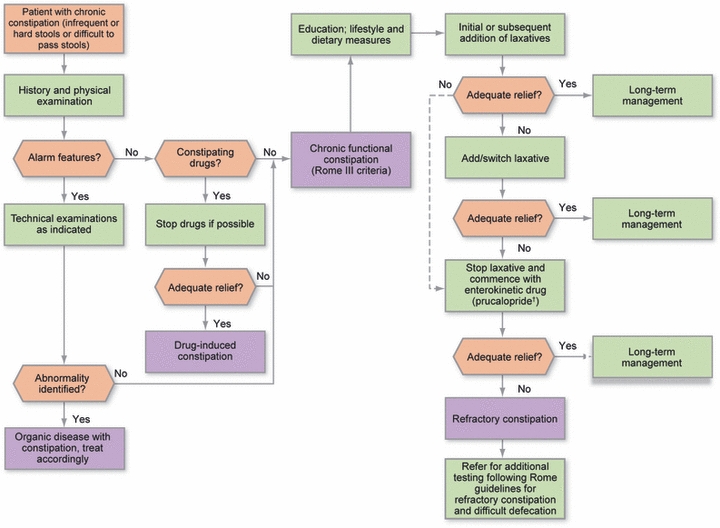
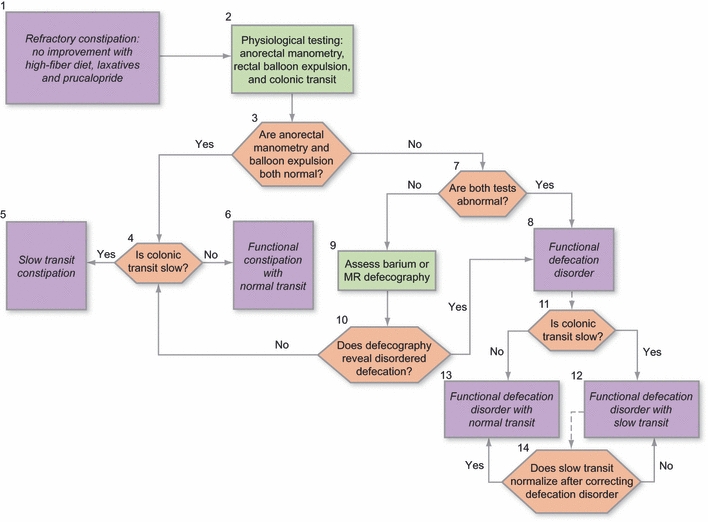
Purpose: We present an overview of the pathophysiology, diagnosis, current management and available guidelines for the treatment of chronic constipation, and include recent data on the efficacy and potential clinical use of the more newly available therapeutic agents. Based on published algorithms and guidelines on the management of chronic constipation, secondary pathologies and causes are first excluded and then diet, lifestyle, and, if available, behavioral measures adopted. If these fail, bulk-forming, osmotic, and stimulant laxatives can be used. If symptoms are not satisfactorily resolved, a prokinetic agent such as prucalopride can be prescribed. Biofeedback is recommended as a treatment for chronic constipation in patients with disordered defecation. Surgery should only be considered once all other treatment options have been exhausted.
© 2011 Blackwell Publishing Ltd.
Figures
Comment in
-
Evolving concepts in chronic constipation in Europe and elsewhere: not worlds apart.Neurogastroenterol Motil. 2011 Aug;23(8):693-6. doi: 10.1111/j.1365-2982.2011.01752.x. Neurogastroenterol Motil. 2011. PMID: 21762282
References
-
- Belsey J, Greenfield S, Candy D, Geraint M. Systematic review: impact of constipation on quality of life in adults and children. Aliment Pharmacol Ther. 2010;31:938–49. - PubMed
-
- Johanson J, Kralstein J. Chronic constipation: a survey of the patient perspective. Aliment Pharmacol Ther. 2007;25:599–608. - PubMed
-
- Wald A, Scarpignato C, Kamm MA, et al. The burden of constipation on quality of life: results of a multinational survey. Aliment Pharmacol Ther. 2007;26:227–36. - PubMed
-
- Tack J, Mueller-Lissner S, Dubois D, Schenck F. Only 27% of European patients with chronic constipation are satisfied with current treatment options. UEGW/WCOG: Gut. 2009;58(Suppl. II)
-
- Pare P, Ferrazzi S, Thompson WG, Irvine EJ, Rance L. An epidemiological survey of constipation in Canada: definitions, rates, demographics, and predictors of health care seeking. Am J Gastroenterol. 2001;96:3130–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
