

(Correcting) misdiagnoses of asthma: a cost effectiveness analysis
- PMID: 21605395
- PMCID: PMC3118954
- DOI: 10.1186/1471-2466-11-27
(Correcting) misdiagnoses of asthma: a cost effectiveness analysis
Abstract
Background: The prevalence of physician-diagnosed-asthma has risen over the past three decades and misdiagnosis of asthma is potentially common.
Objective: to determine whether a secondary-screening-program to establish a correct diagnosis of asthma in those who report a physician diagnosis of asthma is cost effective.
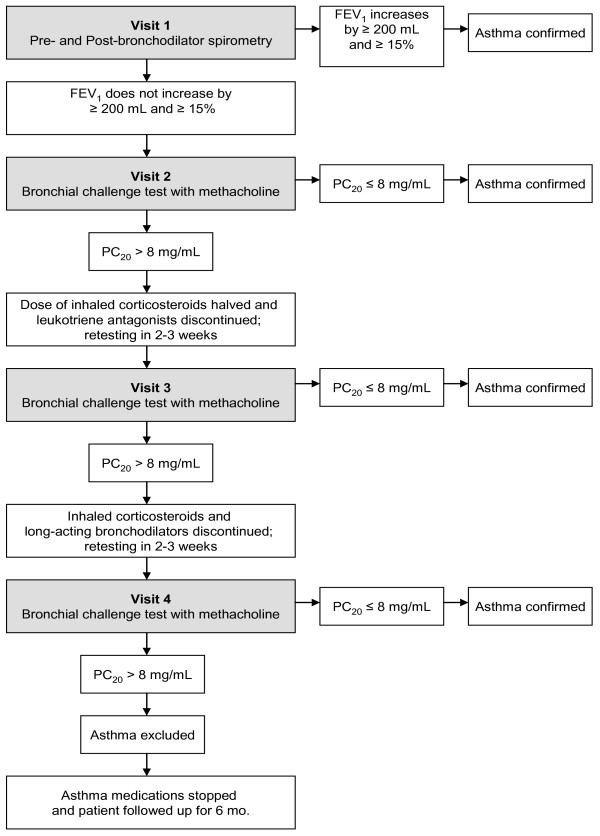
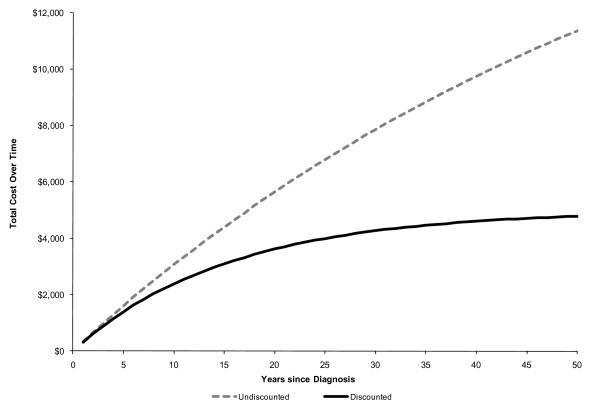
Method: Randomly selected physician-diagnosed-asthmatic subjects from 8 Canadian cities were studied with an extensive diagnostic algorithm to rule-in, or rule-out, a correct diagnosis of asthma. Subjects in whom the diagnosis of asthma was excluded were followed up for 6-months and data on asthma medications and heath care utilization was obtained. Economic analysis was performed to estimate the incremental lifetime costs associated with secondary screening of previously diagnosed asthmatic subjects. Analysis was from the perspective of the Canadian healthcare system and is reported in Canadian dollars.
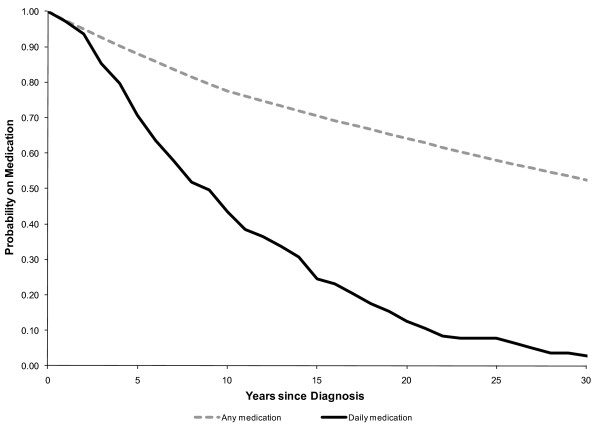
Results: Of 540 randomly selected patients with physician diagnosed asthma 150 (28%; 95%CI 19-37%) did not have asthma when objectively studied. 71% of these misdiagnosed patients were on some asthma medications. Incorporating the incremental cost of secondary-screening for the diagnosis of asthma, we found that the average cost savings per 100 individuals screened was $35,141 (95%CI $4,588-$69,278).
Conclusion: Cost savings primarily resulted from lifetime costs of medication use averted in those who had been misdiagnosed.
Figures
References
-
- National Asthma Survey. 2007. http://www.cdc.gov/nchs/about/major/slaits/nas.htm
-
- Statistics Canada. Persons with asthma, by age and sex. 2009. http://www40.statcan.gc.ca/l01/cst01/health49a-eng.htm?sdi=asthma
-
- Sharpe HM, Sin DD, Andrews EM, Cowie RL, Man P. Alberta Strategy to Help Manage Asthma (ASTHMA): a provincial initiative to improve outcomes for individuals with asthma. Healthc Q. 2004;7(3):55–60. 4. - PubMed
-
- Jin R, Choi BC, Chan BT, McRae L, Li F, Cicutto L. et al.Physician asthma management practices in Canada. Can Respir J. 2000;7(6):456–465. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
