

Integrating intensified case finding of tuberculosis into HIV care: an evaluation from rural Swaziland
- PMID: 21605437
- PMCID: PMC3224363
- DOI: 10.1186/1472-6963-11-118
Integrating intensified case finding of tuberculosis into HIV care: an evaluation from rural Swaziland
Abstract
Background: Swaziland has the highest HIV prevalence in the world and the highest estimated tuberculosis incidence rate in the world. An estimated 80% of TB patients are also infected with HIV. TB detection through intensified case finding (ICF) has yet to become a routine aspect of integrated tuberculosis and HIV care. The purpose of this study was to evaluate implementation of ICF for TB into routine integrated tuberculosis and HIV care at 16 community clinics and one district hospital in Swaziland.
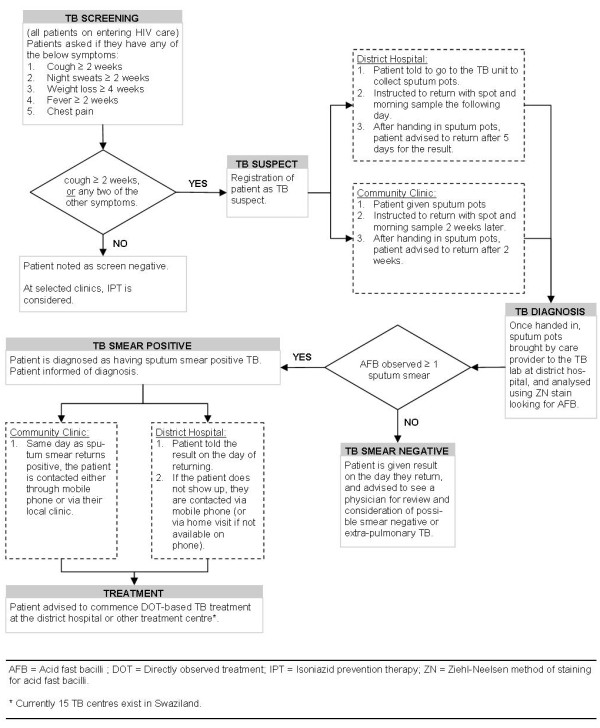
Methods: Nurses and lay counsellors conducted ICF using a TB screening tool and patient pathway at all HIV service entry points in clinics and the hospital. The patient pathway had three-stages; screening, sputum smear diagnosis and TB treatment initiation. Outcomes and losses to follow up were monitored at each stage. Patient demographics, access, and service feasibility and effectiveness were compared at hospital and clinic sites.
Results: 1467 HIV patients at clinics and the hospital were screened over a 3 month period. Large losses to follow up occurred prior to the sputum diagnosis stage; only 47% (n = 172) of TB suspects provided a specimen. 28 cases of smear positive TB were diagnosed and 24 commenced treatment. People screened at clinics were significantly more likely to be female, older, and from rural or geographically remote areas (p < 0.001). There was no significant difference between the hospital and clinics sites in the proportion of all participants screened who were smear positive (x2 = 1.909; p = 0.16). The number needed to screen to detect one sputum positive TB case was 34 at clinics and 63 at the district hospital.
Conclusions: ICF was operationally feasible and became established as a routine aspect of tuberculosis and HIV integrated care. ICF in community clinics was potentially more accessible to an underserved, rural population and was as effective as the hospital service in detecting smear positive TB.
Figures

References
-
- World Health Organisation. WHO Report 2009. Geneva, Switzerland, WHO; 2009. Global tuberculosis control: epidemiology, strategy, financing.
-
- Stop TB Partnership and World Health Organisation. WHO Report 2006. Geneva, Switzerland, WHO; 2006. The Global Plan to Stop TB, 2006-2015.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
