

Supracervical robotic-assisted laparoscopic sacrocolpopexy for pelvic organ prolapse
- PMID: 21605516
- PMCID: PMC3083043
- DOI: 10.4293/108680810X12924466008006
Supracervical robotic-assisted laparoscopic sacrocolpopexy for pelvic organ prolapse
Abstract
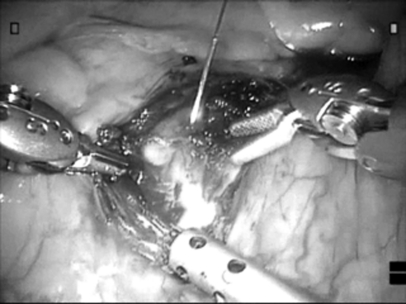
Background: Supracervical robotic-assisted laparoscopic sacrocolpopexy (SRALS) is a new surgical treatment for pelvic organ prolapse that secures the cervical remnant to the sacral promontory. We present our initial experience with SRALS in the same setting as supracervical robotic-assisted hysterectomy (SRAH).
Methods: Women with vaginal vault prolapse and significant apical defects as defined by a Baden-Walker score of greater than or equal to 3 who had not undergone hysterectomy were offered SRALS in combination with SRAH. A chart review was performed to analyze operative and perioperative data. Outcome data also included patients who underwent robotic-assisted laparoscopic sacrocolpopexy (RALS) without any other procedure.
Results: Thirty-three patients underwent RALS, including 12 patients who underwent SRALS. All SRALS were performed following SRAH in the same setting. The mean follow-up for the RALS and SRALS patients was 38.4 months and 20.7 months, respectively. One patient in the RALS group had an apical recurrence. There were no recurrences in the SRALS group.
Conclusions: SRALS is effective for repair of apical vaginal defects in patients with significant pelvic organ prolapse who have not undergone previous hysterectomy. Complications are few and recurrences rare in short- and medium-term follow-up. Greater follow-up and numbers are needed to further establish the role of this procedure.
Figures

Similar articles
-
Robotic laparoendoscopic single-site compared with robotic multi-port sacrocolpopexy for apical compartment prolapse.Am J Obstet Gynecol. 2020 Apr;222(4):358.e1-358.e11. doi: 10.1016/j.ajog.2019.09.048. Epub 2019 Oct 4. Am J Obstet Gynecol. 2020. PMID: 31589864 Clinical Trial.
-
Robotic-assisted laparoscopic sacrocolpopexy for treatment of vaginal vault prolapse.Urology. 2004 Feb;63(2):373-6. doi: 10.1016/j.urology.2003.09.033. Urology. 2004. PMID: 14972496
-
Robot-assisted laparoscopic sacrocolpopexy as management for pelvic organ prolapse.J Endourol. 2009 Apr;23(4):655-8. doi: 10.1089/end.2008.0290. J Endourol. 2009. PMID: 19335154
-
[Laparoscopic sacrocolpopexy for pelvic organ prolapse: guidelines for clinical practice].Prog Urol. 2016 Jul;26 Suppl 1:S27-37. doi: 10.1016/S1166-7087(16)30426-2. Prog Urol. 2016. PMID: 27595624 Review. French.
-
Robotic-assisted sacrocolpopexy for pelvic organ prolapse.Urol Clin North Am. 2014 Nov;41(4):549-57. doi: 10.1016/j.ucl.2014.07.009. Epub 2014 Aug 20. Urol Clin North Am. 2014. PMID: 25306166 Review.
Cited by
-
Robotic pelvic organ prolapse surgery.Nat Rev Urol. 2015 Apr;12(4):216-24. doi: 10.1038/nrurol.2015.51. Epub 2015 Mar 24. Nat Rev Urol. 2015. PMID: 25800401 Review.
-
Robotic Sacrocolpopexy for Treatment of Apical Compartment Prolapse.Int Neurourol J. 2020 Jun;24(2):97-110. doi: 10.5213/inj.2040056.028. Epub 2020 Jun 30. Int Neurourol J. 2020. PMID: 32615671 Free PMC article.
-
Robotic and laparoscopic sacrocolpopexy for pelvic organ prolapse: a systematic review and meta-analysis.Ann Transl Med. 2021 Mar;9(6):449. doi: 10.21037/atm-20-4347. Ann Transl Med. 2021. PMID: 33850846 Free PMC article.
-
Long-term mesh erosion rate following abdominal robotic reconstructive pelvic floor surgery: a prospective study and overview of the literature.Int Urogynecol J. 2020 Jul;31(7):1423-1433. doi: 10.1007/s00192-019-03990-1. Epub 2019 Jun 20. Int Urogynecol J. 2020. PMID: 31222568 Free PMC article. Review.
-
The impact of training residents on the outcome of robotic-assisted sacrocolpopexy.Minim Invasive Surg. 2012;2012:289342. doi: 10.1155/2012/289342. Epub 2012 Nov 1. Minim Invasive Surg. 2012. PMID: 23209891 Free PMC article.
References
-
- Wu JM, Wechter ME, Geller EJ, et al. Hysterectomy rates in the United States, 2003. Obstet Gynecol. 2007; 110: 1091–1095 - PubMed
-
- Reich H, Decaprio J, McGlynn F. Laparoscopic hysterectomy. Gynecol Surg. 1989; 5: 213–216
-
- Reynolds RK, Advincula AP. Robot-assisted laparoscopic hysterectomy: technique and initial experience. Am J Surg. 2006; 191: 555–560 - PubMed
-
- Advincula AP. Surgical techniques: robot-assisted laparoscopic hysterectomy with the da Vinci® surgical system. Int J Med Robotics Comput Assist Surg. 2006; 2: 305–311 - PubMed
-
- Wilcox LS, Koonin LM, Pokras R, et al. Hysterectomy in the United States, 1988 – 1990. Obstet Gynecol. 1994; 83: 549–555 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical