

Myocardial infarction after carotid stenting and endarterectomy: results from the carotid revascularization endarterectomy versus stenting trial
- PMID: 21606394
- PMCID: PMC3173718
- DOI: 10.1161/CIRCULATIONAHA.110.008250
Myocardial infarction after carotid stenting and endarterectomy: results from the carotid revascularization endarterectomy versus stenting trial
Abstract
Background: The Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST) found a higher risk of stroke after carotid artery stenting and a higher risk of myocardial infarction (MI) after carotid endarterectomy.
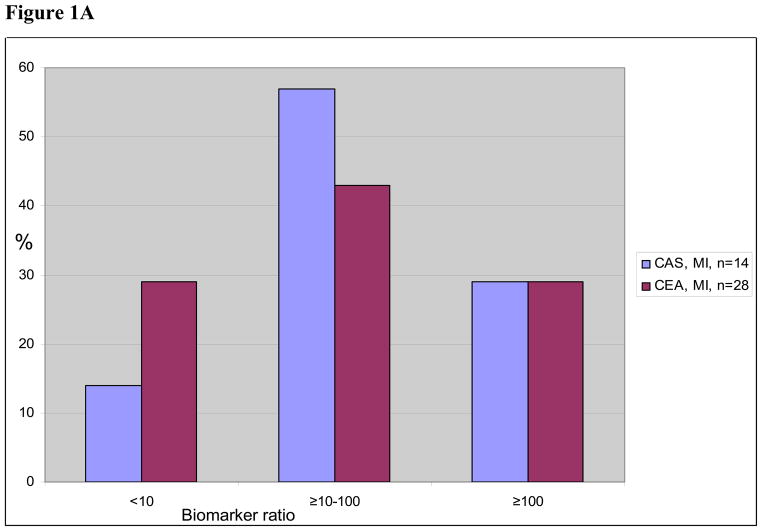
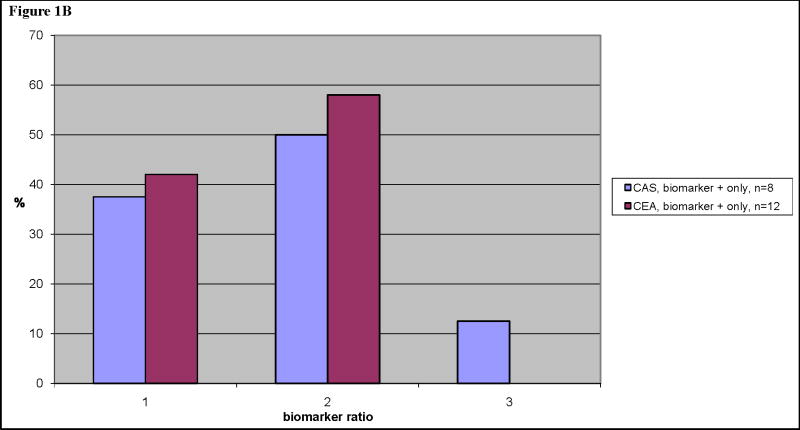
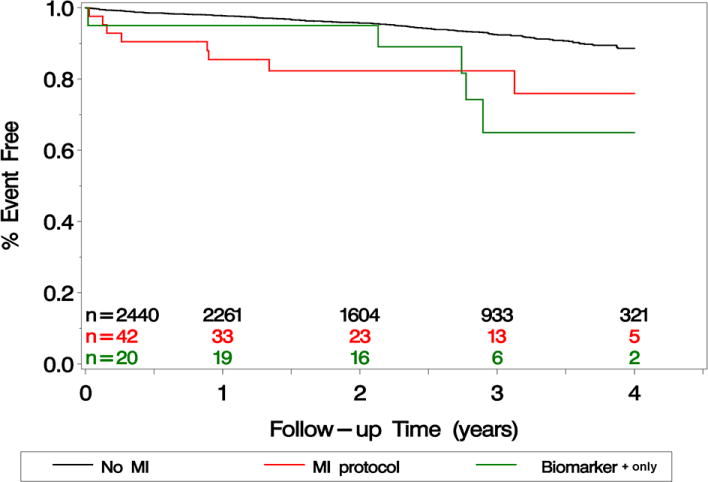
Methods and results: Cardiac biomarkers and ECGs were performed before and 6 to 8 hours after either procedure and if there was clinical evidence of ischemia. In CREST, MI was defined as biomarker elevation plus either chest pain or ECG evidence of ischemia. An additional category of biomarker elevation with neither chest pain nor ECG abnormality was prespecified (biomarker+ only). Crude mortality and risk-adjusted mortality for MI and biomarker+ only were assessed during follow-up. Among 2502 patients, 14 MIs occurred in carotid artery stenting and 28 MIs in carotid endarterectomy (hazard ratio, 0.50; 95% confidence interval, 0.26 to 0.94; P=0.032) with a median biomarker ratio of 40 times the upper limit of normal. An additional 8 carotid artery stenting and 12 carotid endarterectomy patients had biomarker+ only (hazard ratio, 0.66; 95% confidence interval, 0.27 to 1.61; P=0.36), and their median biomarker ratio was 14 times the upper limit of normal. Compared with patients without biomarker elevation, mortality was higher over 4 years for those with MI (hazard ratio, 3.40; 95% confidence interval, 1.67 to 6.92) or biomarker+ only (hazard ratio, 3.57; 95% confidence interval, 1.46 to 8.68). After adjustment for baseline risk factors, both MI and biomarker+ only remained independently associated with increased mortality.
Conclusions: In patients randomized to carotid endarterectomy versus carotid artery stenting, both MI and biomarker+ only were more common with carotid endarterectomy. Although the levels of biomarker elevation were modest, both events were independently associated with increased future mortality and remain an important consideration in choosing the mode of carotid revascularization or medical therapy.
Clinical trial registration: URL: http://www.ClinicalTrials.gov. Unique identifier: NCT00004732.
Figures
Comment in
-
Fire in the hole: carotid stenting versus endarterectomy.Circulation. 2011 Jun 7;123(22):2522-5. doi: 10.1161/CIRCULATIONAHA.111.034314. Epub 2011 May 23. Circulation. 2011. PMID: 21606395 No abstract available.
References
-
- Brott TG, Hobson RW, II, Howard G, Roubin GS, Clark WM, Brooks W, Mackey A, Hill MD, Leimgruber PP, Sheffet AJ, Howard VJ, Moore WS, Voeks JH, Hopkins LN, Cutlip DE, Cohen DJ, Popma JJ, Ferguson RD, Cohen SN, Blackshear JL, Silver FL, Mohr JP, Lal BK, Meschia JF. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med. 2010;363:11–23. - PMC - PubMed
-
- Davis SM, Donnan GA. Carotid-artery stenting in stroke prevention. N Engl J Med. 2010;363:800–82. - PubMed
-
- Kim LJ, Martinez EA, Faraday N, Dorman T, Fleisher LA, Perler BA, Williams GM, Chan D, Pronovost PJ. Cardiac troponin I predicts short-term mortality in vascular surgery patients. Circ. 2002;106:2366–2371. - PubMed
-
- Landesberg G, Shatz V, Akopnik I, Wolf YG, Mayer M, Berlatzky Y, Weissman C, Mosseri M. Association of cardiac troponin, CK-MB, and postoperative survival after major vascular surgery. J Am Coll Cardiol. 2003;42:1547–54. - PubMed
-
- Oscarsson A, Eintrei C, Anskar S, Engdahl O, Fagerstrom L, Blomquist P, Fredriksson M, Swahn E. Troponin T-values provide long-term prognosis in elderly patients undergoing non-cardiac surgery. Acta Anaesth Scand. 2004:1071–1079. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
