

Cancer-immune equilibrium: questions unanswered
- PMID: 21607751
- PMCID: PMC3170416
- DOI: 10.1007/s12307-011-0065-8
Cancer-immune equilibrium: questions unanswered
Abstract
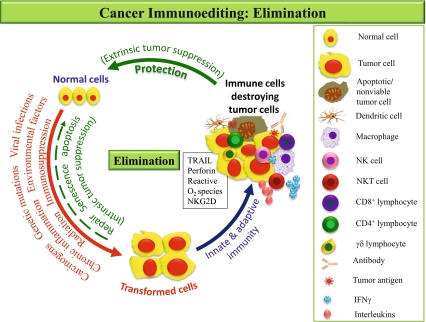
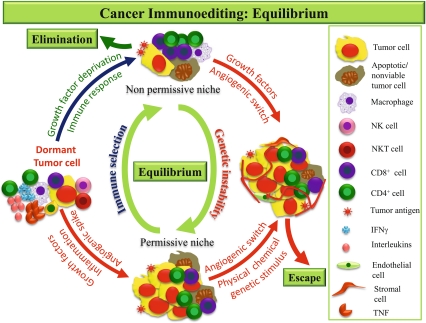
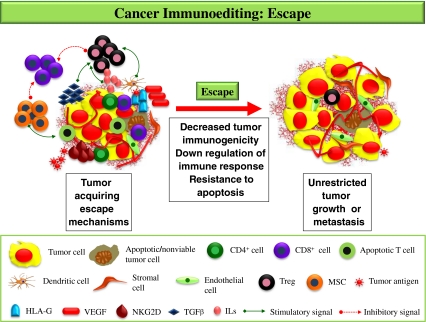
Cancer-immune (CI) equilibrium constitutes an important component of the cancer immunoediting theory. It is defined as a period during which our immune system and cancer live in harmony in the body. The immune system, though not able to completely eliminate the cancer, doesn't allow it to progress or metastasize further. Mechanisms of this phase are poorly understood because this phase is difficult to identify even by the most modern detection methods. Till now, the work done on the equilibrium phase of cancer, suggests promising improvements in cancer therapy if the disease could be withheld in this phase. However, there are many queries which remain to be addressed about this interesting yet unresolved phase of cancer immunity.
Figures
References
LinkOut - more resources
Full Text Sources
