

Influence of preceding length of anticoagulant treatment and initial presentation of venous thromboembolism on risk of recurrence after stopping treatment: analysis of individual participants' data from seven trials
- PMID: 21610040
- PMCID: PMC3100759
- DOI: 10.1136/bmj.d3036
Influence of preceding length of anticoagulant treatment and initial presentation of venous thromboembolism on risk of recurrence after stopping treatment: analysis of individual participants' data from seven trials
Abstract
Objective: To determine how length of anticoagulation and clinical presentation of venous thromboembolism influence the risk of recurrence after anticoagulant treatment is stopped and to identify the shortest length of anticoagulation that reduces the risk of recurrence to its lowest level.
Design: Pooled analysis of individual participants' data from seven randomised trials.
Setting: Outpatient anticoagulant clinics in academic centres.
Population: 2925 men or women with a first venous thromboembolism who did not have cancer and received different durations of anticoagulant treatment.
Main outcome measure: First recurrent venous thromboembolism after stopping anticoagulant treatment during up to 24 months of follow-up.
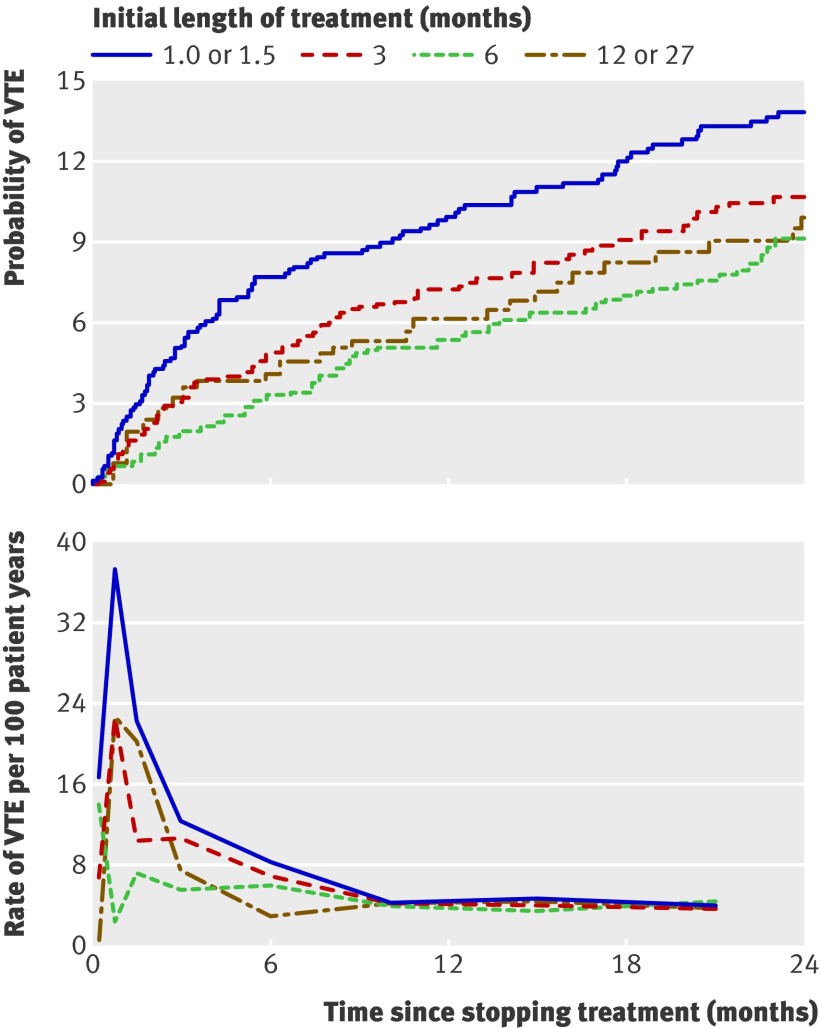
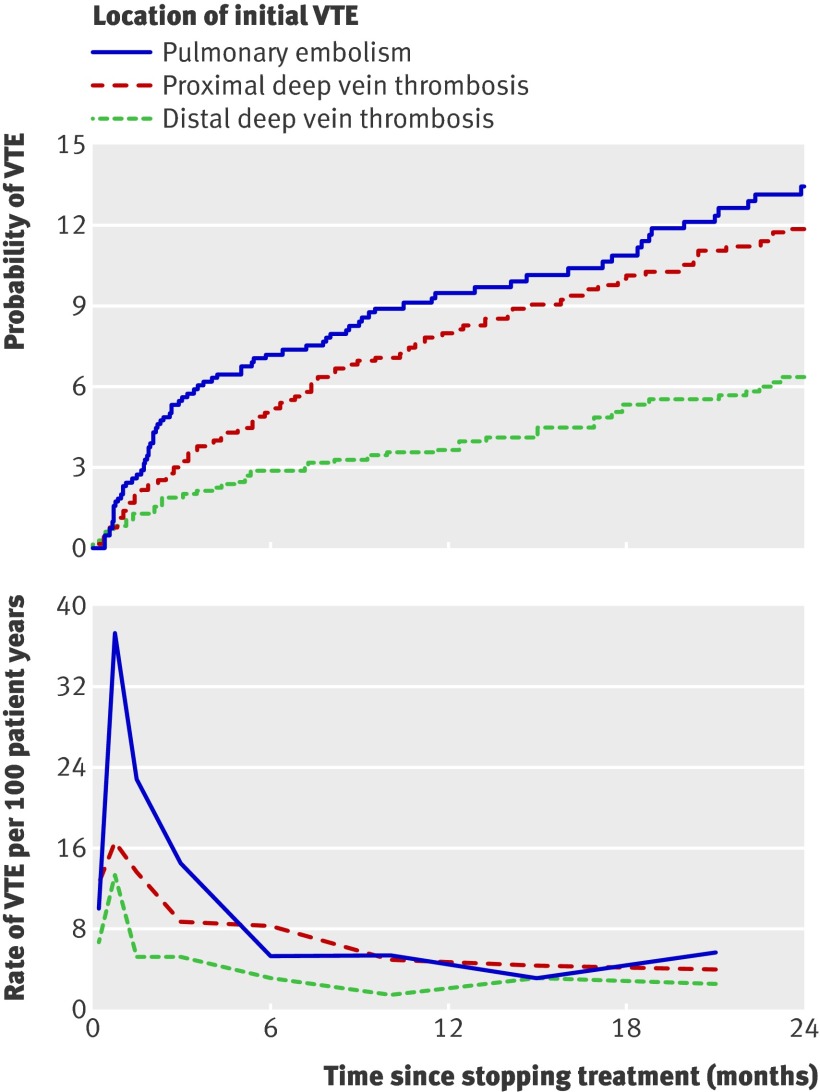
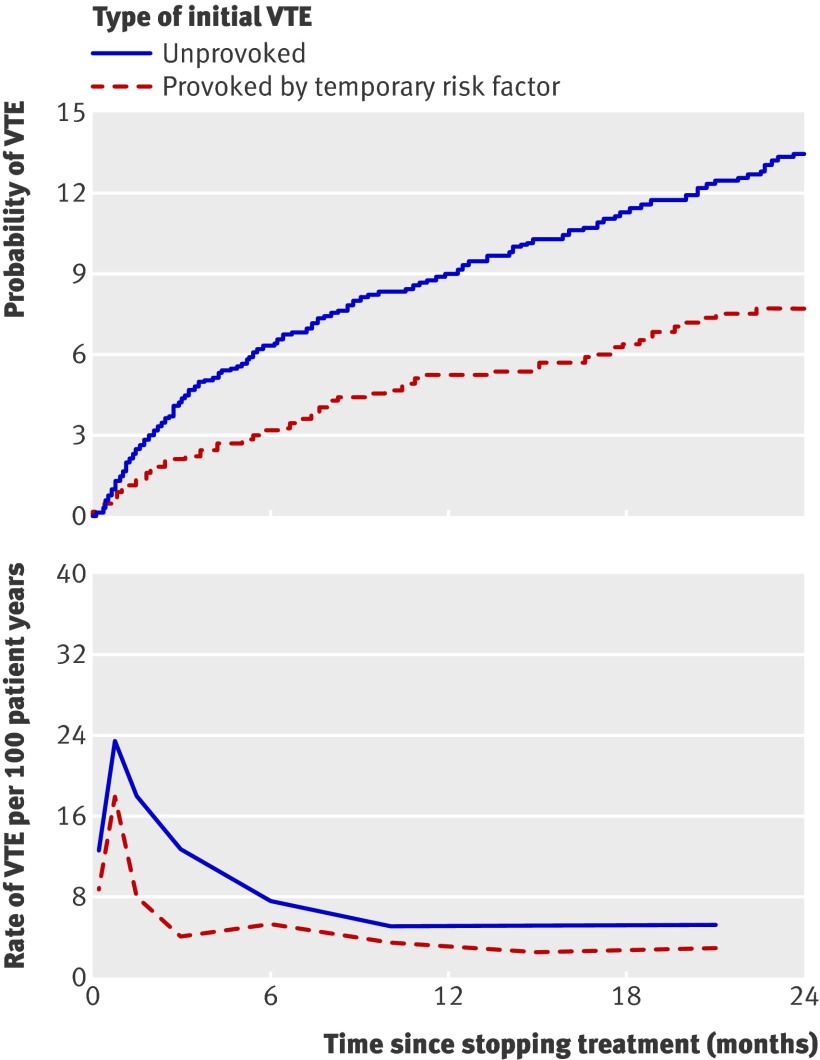
Results: Recurrence was lower after isolated distal deep vein thrombosis than after proximal deep vein thrombosis (hazard ratio 0.49, 95% confidence interval 0.34 to 0.71), similar after pulmonary embolism and proximal deep vein thrombosis (1.19, 0.87 to 1.63), and lower after thrombosis provoked by a temporary risk factor than after unprovoked thrombosis (0.55, 0.41 to 0.74). Recurrence was higher if anticoagulation was stopped at 1.0 or 1.5 months compared with at 3 months or later (hazard ratio 1.52, 1.14 to 2.02) and similar if treatment was stopped at 3 months compared with at 6 months or later (1.19, 0.86 to 1.65). High rates of recurrence associated with shorter durations of anticoagulation were confined to the first 6 months after stopping treatment.
Conclusion: Three months of treatment achieves a similar risk of recurrent venous thromboembolism after stopping anticoagulation to a longer course of treatment. Unprovoked proximal deep vein thrombosis and pulmonary embolism have a high risk of recurrence whenever treatment is stopped.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Duration of anticoagulation for venous thromboembolism.BMJ. 2011 May 24;342:d2758. doi: 10.1136/bmj.d2758. BMJ. 2011. PMID: 21610039 No abstract available.
-
Venous thromboembolism: optimal therapy duration assessed.Nat Rev Cardiol. 2011 Jun 7;8(7):362. doi: 10.1038/nrcardio.2011.90. Nat Rev Cardiol. 2011. PMID: 21647181 No abstract available.
-
[No difference in recurrence risk of venous thromboembolism treated with anticoagulation for 3 months or longer].Praxis (Bern 1994). 2011 Nov 16;100(23):1431-2. doi: 10.1024/1661-8157/a000729. Praxis (Bern 1994). 2011. PMID: 22086383 German. No abstract available.
References
-
- Kearon C, Kahn SR, Agnelli G, Goldhaber S, Raskob G, Comerota AJ. Antithrombotic therapy for venous thromboembolic disease: ACCP evidence-based clinical practice guidelines (8th ed). Chest 2008;133:454-545S. - PubMed
-
- Research Committee of the British Thoracic Society. Optimum duration of anticoagulation for deep-vein thrombosis and pulmonary embolism. Lancet 1992;340:873-6. - PubMed
-
- Levine MN, Hirsh J, Gent M, Turpie AG, Weitz J, Ginsberg J, et al. Optimal duration of oral anticoagulant therapy: a randomized trial comparing four weeks with three months of warfarin in patients with proximal deep vein thrombosis. Thromb Haemost 1995;74:606-11. - PubMed
-
- Schulman S, Rhedin A-S, Lindmarker P, Carlsson A, Lärfars G, Nicol P, et al. A comparison of six weeks with six months of oral anticoagulant therapy after a first episode of venous thromboembolism. N Engl J Med 1995;332:1661-5. - PubMed
-
- Schulman S, Granqvist S, Holmstrom M, Carlsson A, Lindmarker P, Nicol P, et al. The duration of oral anticoagulant therapy after a second episode of venous thromboembolism. N Engl J Med 1997;336:393-8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical