

Impact of therapeutic hypothermia onset and duration on survival, neurologic function, and neurodegeneration after cardiac arrest
- PMID: 21610611
- PMCID: PMC3102228
- DOI: 10.1097/CCM.0b013e318212020a
Impact of therapeutic hypothermia onset and duration on survival, neurologic function, and neurodegeneration after cardiac arrest
Abstract
Objective: Post-cardiac-arrest therapeutic hypothermia improves outcomes in comatose cardiac arrest survivors. This study tests the hypothesis that the efficacy of post-cardiac-arrest therapeutic hypothermia is dependent on the onset and duration of therapy.
Design: Prospective randomized laboratory investigation.
Setting: University research laboratory.
Subjects: A total of 268 male Long Evans rats.
Interventions: Post-cardiac-arrest therapeutic hypothermia.
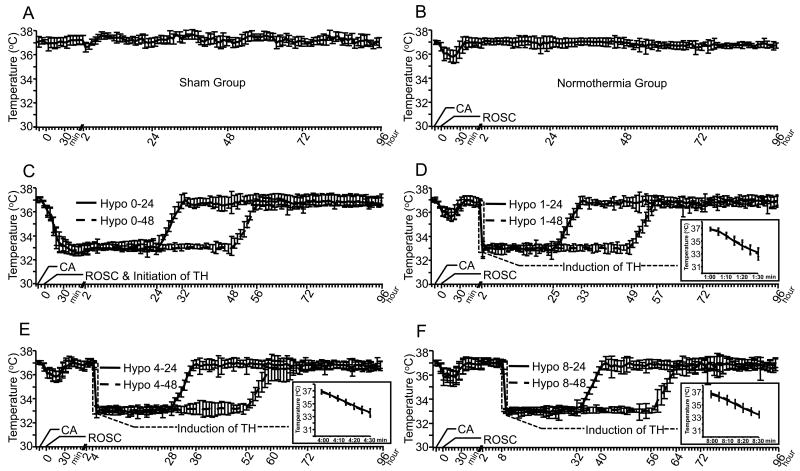
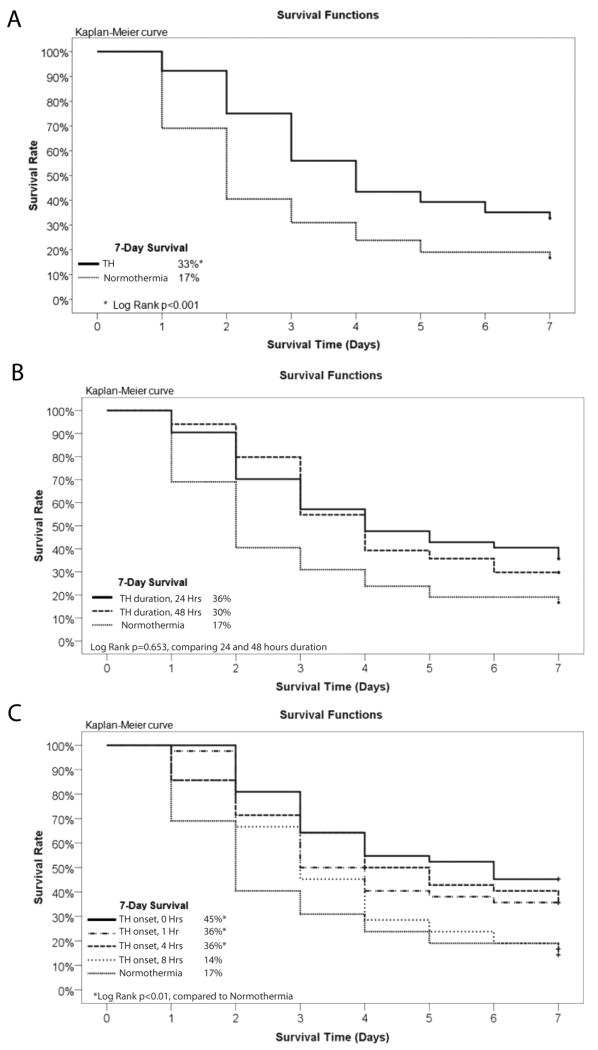
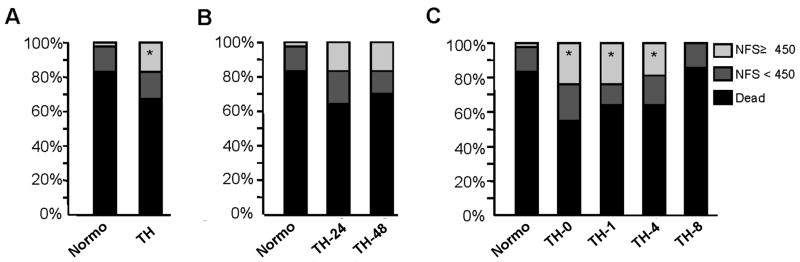
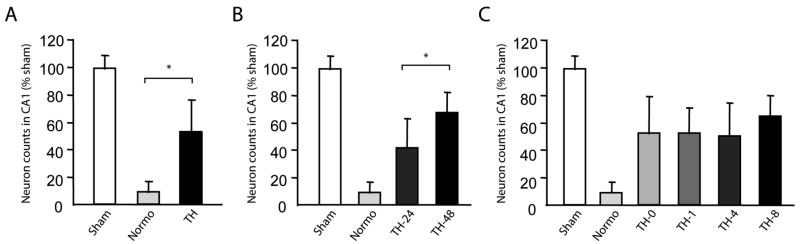
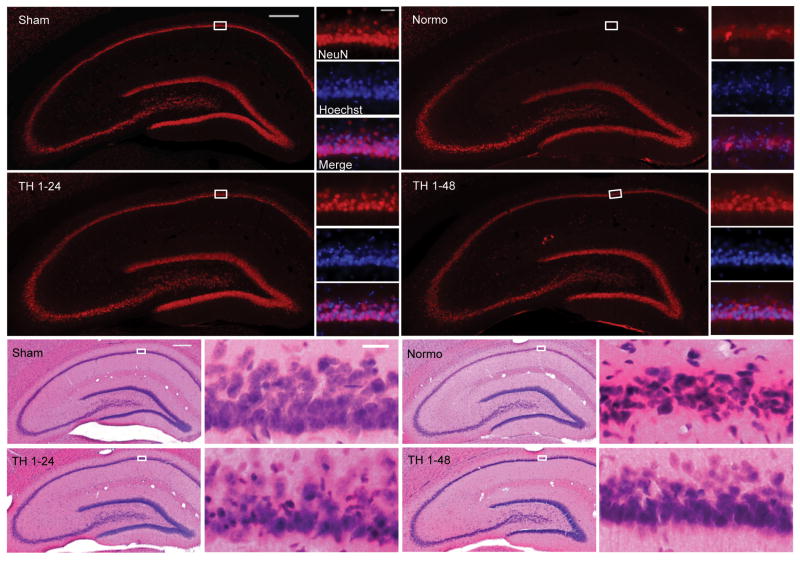
Measurements and main results: Adult male Long Evans rats that achieved return of spontaneous circulation after a 10-min asphyxial cardiac arrest were block randomized to normothermia (37°C ± 1°C) or therapeutic hypothermia (33°C ± 1°C) initiated 0, 1, 4, or 8 hrs after return of spontaneous circulation and maintained for 24 or 48 hrs. Therapeutic hypothermia initiated 0, 1, 4, and 8 hrs after return of spontaneous circulation resulted in 7-day survival rates of 45%*, 36%*, 36%*, and 14%, respectively, compared to 17% for normothermic controls and survival with good neurologic function rates of 24%*, 24%*, 19%*, and 0%, respectively, compared to 2% for normothermic controls (*p < .05 vs. normothermia). These outcomes were not different when therapeutic hypothermia was maintained for 24 vs. 48 hrs. In contrast, hippocampal CA1 pyramidal neuron counts were 53% ± 27%*, 53% ± 19%*, 51% ± 24%*, and 65% ± 16%* of normal, respectively, when therapeutic hypothermia was initiated 0, 1, 4, or 8 hrs after return of spontaneous circulation compared to 9% in normothermic controls (*p < .01 vs. normothermia). Furthermore, surviving neuron counts were greater when therapeutic hypothermia was maintained for 48 hrs compared to 24 hrs (68% ± 15%* vs. 42% ± 22%, *p < .0001).
Conclusions: In this study, post-cardiac-arrest therapeutic hypothermia resulted in comparable improvement of survival and survival with good neurologic function when initiated within 4 hrs after return of spontaneous circulation. However, histologic assessment of neuronal survival revealed a potentially broader therapeutic window and greater neuroprotection when therapeutic hypothermia was maintained for 48 vs. 24 hrs.
Conflict of interest statement
The remaining authors have not disclosed any potential conflicts of interest.
Figures
Comment in
-
Therapeutic hypothermia after cardiac arrest: it's about time.Crit Care Med. 2011 Jun;39(6):1586-7. doi: 10.1097/CCM.0b013e31821856a9. Crit Care Med. 2011. PMID: 21610638 No abstract available.
References
-
- Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutteridge G, Smith K. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346:557–563. - PubMed
-
- Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:549–556. - PubMed
-
- Peberdy MA, Callaway CW, Neumar RW, Geocadin RG, Zimmerman JL, Donnino M, Gabrielli A, Silvers SM, Zaritsky AL, Merchant R, Vanden Hoek TL, Kronick SL. Part 9: post-cardiac arrest care: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18 Suppl 3):S768–S786. - PubMed
-
- Kuboyama K, Safar P, Radovsky A, Tisherman SA, Stezoski SW, Alexander H. Delay in cooling negates the beneficial effect of mild resuscitative cerebral hypothermia after cardiac arrest in dogs: a prospective, randomized study. Crit Care Med. 1993;21:1348–1358. - PubMed
-
- Takata K, Takeda Y, Sato T, Nakatsuka H, Yokoyama M, Morita K. Effects of hypothermia for a short period on histologic outcome and extracellular glutamate concentration during and after cardiac arrest in rats. Crit Care Med. 2005;33:1340–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
