

Incidence and risk factors of serious adverse events during antituberculous treatment in Rwanda: a prospective cohort study
- PMID: 21611117
- PMCID: PMC3097195
- DOI: 10.1371/journal.pone.0019566
Incidence and risk factors of serious adverse events during antituberculous treatment in Rwanda: a prospective cohort study
Abstract
Background: Tuberculosis (TB) and TB-human immunodeficiency virus infection (HIV) coinfection is a major public health concern in resource-limited settings. Although TB treatment is challenging in HIV-infected patients because of treatment interactions, immunopathological reactions, and concurrent infections, few prospective studies have addressed this in sub-Saharan Africa. In this study we aimed to determine incidence, causes of, and risk factors for serious adverse events among patients on first-line antituberculous treatment, as well as its impact on antituberculous treatment outcome.
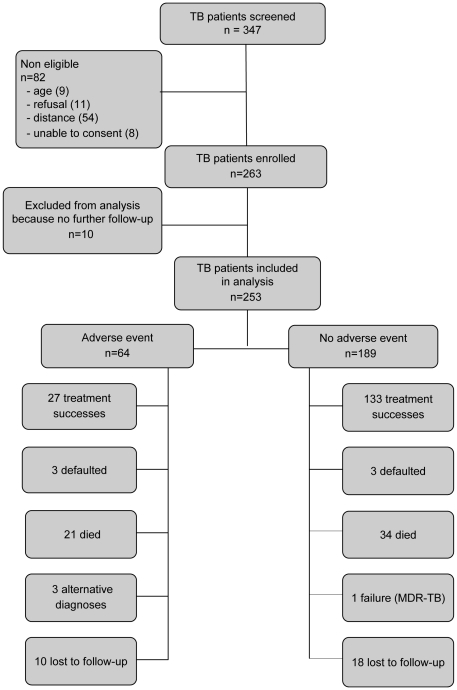
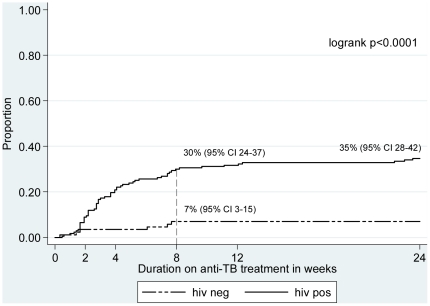
Methods and findings: Prospective observational cohort study of adults treated for TB at the Internal Medicine department of the Kigali University Hospital from May 2008 through August 2009. Of 263 patients enrolled, 253 were retained for analysis: median age 35 (Interquartile range, IQR 28-40), 55% male, 66% HIV-positive with a median CD4 count 104 cells/mm(3) (IQR 44-248 cells/mm(3)). Forty percent had pulmonary TB, 43% extrapulmonary TB and 17% a mixed form. Sixty-four (26%) developed a serious adverse event; 58/167 (35%) HIV-infected vs. 6/86 (7%) HIV-uninfected individuals. Commonest events were concurrent infection (n = 32), drug-induced hepatitis (n = 24) and paradoxical reactions/TB-IRIS (n = 23). HIV-infection (adjusted Hazard Ratio, aHR 3.4, 95% Confidence Interval, CI 1.4-8.7) and extrapulmonary TB (aHR 2, 95%CI 1.1-3.7) were associated with an increased risk of serious adverse events. For TB/HIV co-infected patients, extrapulmonary TB (aHR 2.0, 95%CI 1.1-3.9) and CD4 count <100 cells/mm3 at TB diagnosis (aHR 1.7, 95%CI 1.0-2.9) were independent predictors. Adverse events were associated with an almost two-fold higher risk of unsuccessful treatment outcome at 6 months (HR 1.89, 95%CI 1.3-3.0).
Conclusion: Adverse events frequently complicate the course of antituberculous treatment and worsen treatment outcome, particularly in patients with extrapulmonary TB and advanced immunodeficiency. Concurrent infection accounts for most events. Our data suggest that deterioration in a patient already receiving antituberculous treatment should prompt an aggressive search for additional infections.
Conflict of interest statement
Figures
References
-
- Dean GL, Edwards SG, Ives NJ, Matthews G, Fox EF, et al. Treatment of tuberculosis in HIV-infected persons in the era of highly active antiretroviral therapy. AIDS. 2002;16:75–83. - PubMed
-
- Yee D, Valiquette C, Pelletier M, Parisien I, Rocher I, et al. Incidence of serious side effects from first-line antituberculosis drugs among patients treated for active tuberculosis. Am J Respir Crit Care Med. 2003;167:1472–1477. - PubMed
-
- Lanternier F, Dalban C, Perez L, Bricaire F, Costagliola D, et al. Tolerability of anti-tuberculosis treatment and HIV serostatus. Int J Tuberc Lung Dis. 2007;11:1203–1209. - PubMed
-
- Marks DJ, Dheda K, Dawson R, Ainslie G, Miller RF. Adverse events to antituberculosis therapy: influence of HIV and antiretroviral drugs. Int J STD AIDS. 2009;20:339–345. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
