

Selective venous catheterization for the localization of phosphaturic mesenchymal tumors
- PMID: 21611969
- PMCID: PMC3179290
- DOI: 10.1002/jbmr.316
Selective venous catheterization for the localization of phosphaturic mesenchymal tumors
Abstract
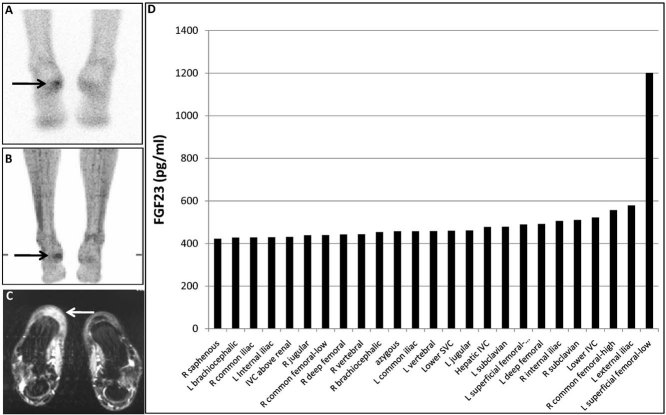
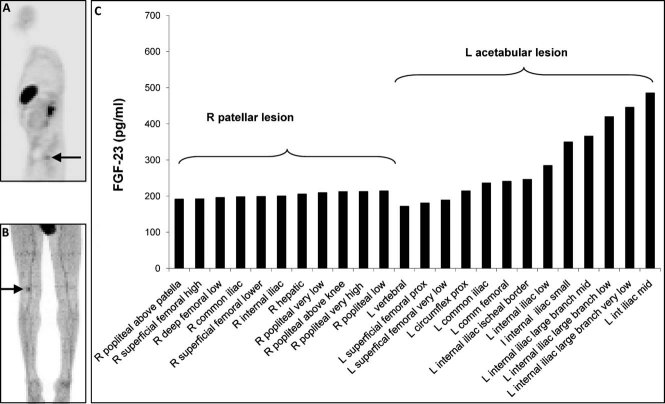
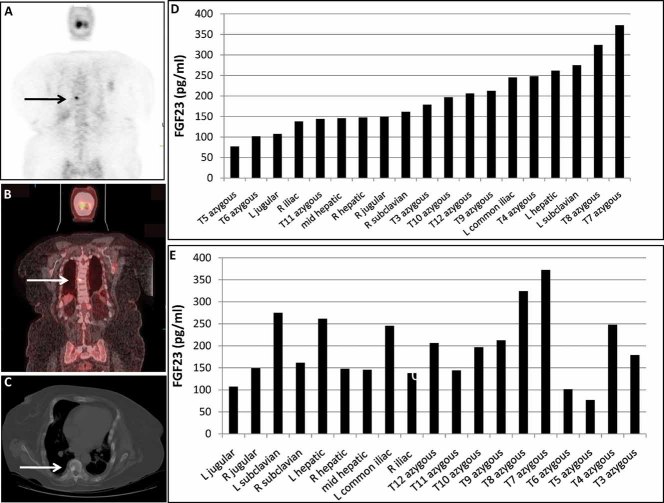
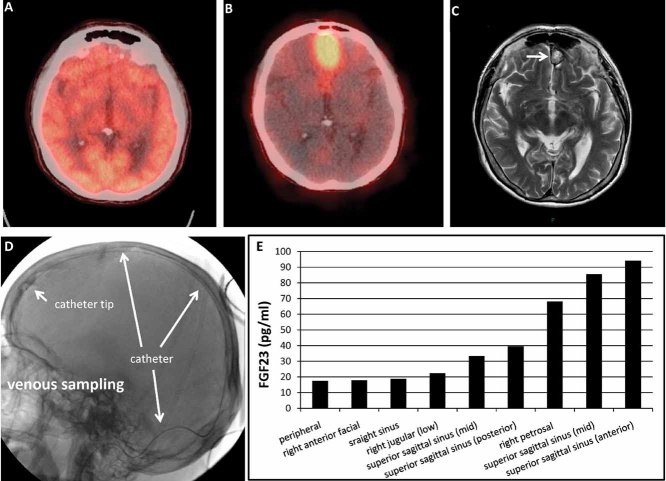
Tumor-induced osteomalacia (TIO) is characterized by renal phosphate wasting, hypophosphatemia, and aberrant vitamin D(3) metabolism and is caused by fibroblast growth factor 23 (FGF-23)-producing mesenchymal tumors, which are often difficult to locate. We investigated the utility of selective venous sampling in tumor localization. The primary endpoint was identification of the FGF-23 concentration ratio between the venous drainage of the tumor bed and the general circulation that was diagnostic of the location of an FGF-23-secreting tumor. Fourteen subjects underwent 15 sampling procedures after functional and anatomic imaging studies. Subjects fit into three imaging categories: no suspicious site, multiple sites, and single site (positive controls). FGF-23 levels were measured by ELISA. Suspicious tumors were resected for diagnosis, confirmation, and cure. In subjects with a positive venous sampling study and subsequent cure, a minimum ratio of 1.6 was diagnostic. In 7 of 14 subjects there was suggestive imaging, a diagnostic ratio, and an associated TIO tumor (true positive). Four of these required complicated resection procedures. In 4 of 14 subjects with no suspicious site on imaging studies, an FGF-23 diagnostic ratio was not detected (true negative). Biopsy or resection of a single lesion in 2 of 14 subjects with a diagnostic ratio failed to identify a TIO tumor (false positive). A diagnostic FGF-23 ratio was absent in 1 of 14 subjects whose tumor was a single highly suspicious lesion on imaging studies (false negative). These data yield a sensitivity of 0.87 [95% confidence interval (CI) 0.47-0.99] and a specificity of 0.71 (95% CI 0.29-0.96). Selective venous sampling for FGF-23 was particularly useful in subjects with multiple suspicious sites or an anatomically challenging planned resection but not in the absence of a suspicious lesion on imaging studies.
Copyright © 2011 American Society for Bone and Mineral Research.
Figures
References
-
- Drezner MK. PHEX gene and hypophosphatemia. Kidney Int. 2000;57:9–18. - PubMed
-
- Jan de Beur SM. Tumor-induced osteomalacia. JAMA. 2005;294:1260–1267. - PubMed
-
- Jonsson KB, Zahradnik R, Larsson T, et al. Fibroblast growth factor 23 in oncogenic osteomalacia and X-linked hypophosphatemia. N Engl J Med. 2003;348:1656–1663. - PubMed
-
- Folpe AL, Fanburg-Smith JC, Billings SD, et al. Most osteomalacia-associated mesenchymal tumors are a single histopathologic entity: an analysis of 32 cases and a comprehensive review of the literature. Am J Surg Pathol. 2004;28:1–30. - PubMed
-
- Autosomal dominant hypophosphataemic rickets is associated with mutations in FGF-23. Nat Genet. 2000;26:345–348. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
