

Abiraterone and increased survival in metastatic prostate cancer
- PMID: 21612468
- PMCID: PMC3471149
- DOI: 10.1056/NEJMoa1014618
Abiraterone and increased survival in metastatic prostate cancer
Abstract
Background: Biosynthesis of extragonadal androgen may contribute to the progression of castration-resistant prostate cancer. We evaluated whether abiraterone acetate, an inhibitor of androgen biosynthesis, prolongs overall survival among patients with metastatic castration-resistant prostate cancer who have received chemotherapy.
Methods: We randomly assigned, in a 2:1 ratio, 1195 patients who had previously received docetaxel to receive 5 mg of prednisone twice daily with either 1000 mg of abiraterone acetate (797 patients) or placebo (398 patients). The primary end point was overall survival. The secondary end points included time to prostate-specific antigen (PSA) progression (elevation in the PSA level according to prespecified criteria), progression-free survival according to radiologic findings based on prespecified criteria, and the PSA response rate.
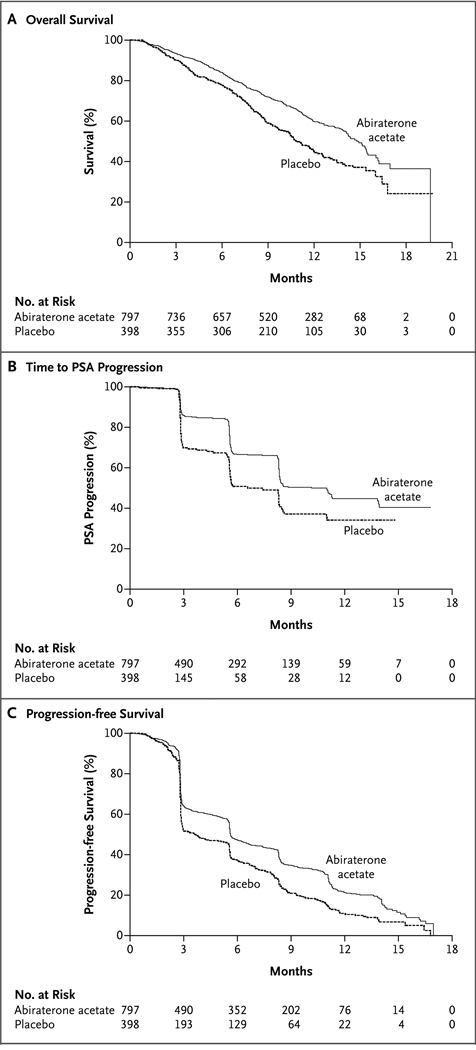
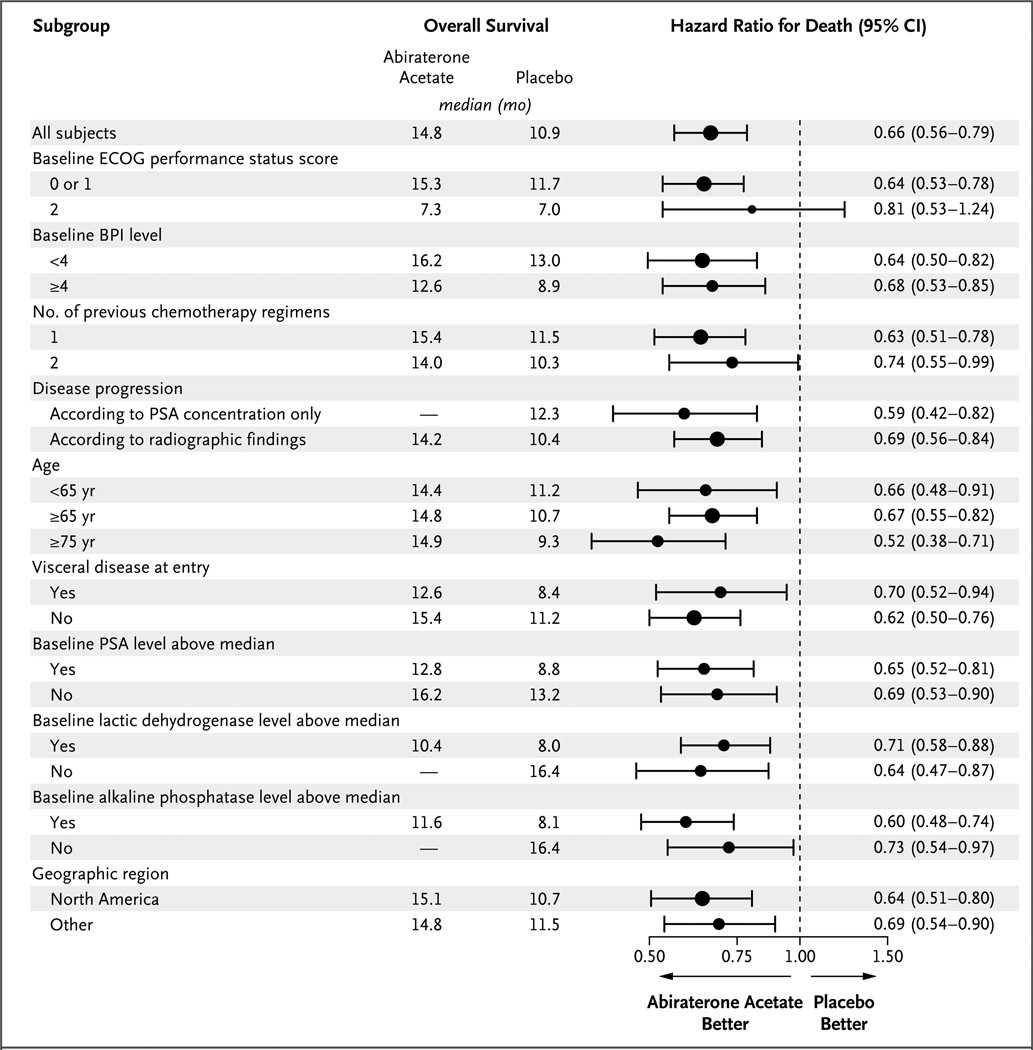
Results: After a median follow-up of 12.8 months, overall survival was longer in the abiraterone acetate-prednisone group than in the placebo-prednisone group (14.8 months vs. 10.9 months; hazard ratio, 0.65; 95% confidence interval, 0.54 to 0.77; P<0.001). Data were unblinded at the interim analysis, since these results exceeded the preplanned criteria for study termination. All secondary end points, including time to PSA progression (10.2 vs. 6.6 months; P<0.001), progression-free survival (5.6 months vs. 3.6 months; P<0.001), and PSA response rate (29% vs. 6%, P<0.001), favored the treatment group. Mineralocorticoid-related adverse events, including fluid retention, hypertension, and hypokalemia, were more frequently reported in the abiraterone acetate-prednisone group than in the placebo-prednisone group.
Conclusions: The inhibition of androgen biosynthesis by abiraterone acetate prolonged overall survival among patients with metastatic castration-resistant prostate cancer who previously received chemotherapy. (Funded by Cougar Biotechnology; COU-AA-301 ClinicalTrials.gov number, NCT00638690.).
Figures
Comment in
-
Expanding treatment options for metastatic prostate cancer.N Engl J Med. 2011 May 26;364(21):2055-8. doi: 10.1056/NEJMe1102758. N Engl J Med. 2011. PMID: 21612475 Free PMC article. No abstract available.
-
Beefing up prostate cancer therapy with performance-enhancing (anti-) steroids.Cancer Cell. 2011 Jul 12;20(1):7-9. doi: 10.1016/j.ccr.2011.06.019. Cancer Cell. 2011. PMID: 21741594 Free PMC article.
-
Prostate cancer: Abiraterone increases overall survival in men with castration-resistant prostate cancer.Nat Rev Urol. 2011 Jul 8;8(7):351. doi: 10.1038/nrurol.2011.94. Nat Rev Urol. 2011. PMID: 21743442 No abstract available.
-
Combination therapy: Abiraterone prolongs survival in metastatic prostate cancer.Nat Rev Clin Oncol. 2011 Aug 2;8(9):515-6. doi: 10.1038/nrclinonc.2011.111. Nat Rev Clin Oncol. 2011. PMID: 21808270
-
Abiraterone and increased survival in metastatic prostate cancer.N Engl J Med. 2011 Aug 25;365(8):766-7; author reply 767-8. doi: 10.1056/NEJMc1107198. N Engl J Med. 2011. PMID: 21864181 No abstract available.
-
Abiraterone and increased survival in metastatic prostate cancer.N Engl J Med. 2011 Aug 25;365(8):766; author reply 767-8. doi: 10.1056/NEJMc1107198. N Engl J Med. 2011. PMID: 21864182 No abstract available.
-
Re: Abiraterone and increased survival in metastatic prostate cancer.J Urol. 2011 Dec;186(6):2253-4. doi: 10.1016/j.juro.2011.08.042. Epub 2011 Oct 22. J Urol. 2011. PMID: 22078584 No abstract available.
-
Words of wisdom. Re: Abiraterone and increased survival in metastatic prostate cancer.Eur Urol. 2012 Apr;61(4):850. doi: 10.1016/j.eururo.2012.01.036. Eur Urol. 2012. PMID: 22373884 No abstract available.
References
-
- Hellerstedt BA, Pienta KJ. The current state of hormonal therapy for prostate cancer. CA Cancer J Clin. 2002;52:154–179. - PubMed
-
- Scher HI, Sawyers CL. Biology of progressive, castration-resistant prostate cancer: directed therapies targeting the androgen-receptor signaling axis. J Clin Oncol. 2005;23:8253–8261. - PubMed
-
- Lam JS, Leppert JT, Vemulapalli SN, Shvarts O, Belldegrun AS. Secondary hormonal therapy for advanced prostate cancer. J Urol. 2006;175:27–34. - PubMed
-
- Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med. 2004;351:1502–1512. - PubMed
-
- de Bono JS, Oudard S, Ozguroglu M, et al. Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: a randomised open-label trial. Lancet. 2010;376:1147–1154. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous