

Body-weight-supported treadmill rehabilitation after stroke
- PMID: 21612471
- PMCID: PMC3175688
- DOI: 10.1056/NEJMoa1010790
Body-weight-supported treadmill rehabilitation after stroke
Abstract
Background: Locomotor training, including the use of body-weight support in treadmill stepping, is a physical therapy intervention used to improve recovery of the ability to walk after stroke. The effectiveness and appropriate timing of this intervention have not been established.
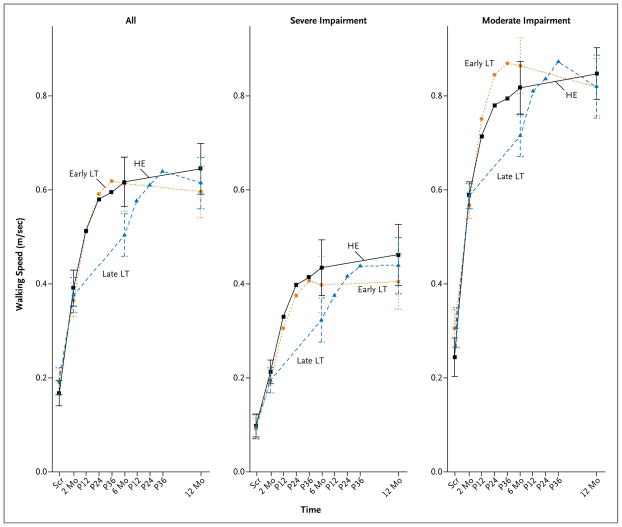
Methods: We stratified 408 participants who had had a stroke 2 months earlier according to the extent of walking impairment--moderate (able to walk 0.4 to <0.8 m per second) or severe (able to walk <0.4 m per second)--and randomly assigned them to one of three training groups. One group received training on a treadmill with the use of body-weight support 2 months after the stroke had occurred (early locomotor training), the second group received this training 6 months after the stroke had occurred (late locomotor training), and the third group participated in an exercise program at home managed by a physical therapist 2 months after the stroke (home-exercise program). Each intervention included 36 sessions of 90 minutes each for 12 to 16 weeks. The primary outcome was the proportion of participants in each group who had an improvement in functional walking ability 1 year after the stroke.
Results: At 1 year, 52.0% of all participants had increased functional walking ability. No significant differences in improvement were found between early locomotor training and home exercise (adjusted odds ratio for the primary outcome, 0.83; 95% confidence interval [CI], 0.50 to 1.39) or between late locomotor training and home exercise (adjusted odds ratio, 1.19; 95% CI, 0.72 to 1.99). All groups had similar improvements in walking speed, motor recovery, balance, functional status, and quality of life. Neither the delay in initiating the late locomotor training nor the severity of the initial impairment affected the outcome at 1 year. Ten related serious adverse events were reported (occurring in 2.2% of participants undergoing early locomotor training, 3.5% of those undergoing late locomotor training, and 1.6% of those engaging in home exercise). As compared with the home-exercise group, each of the groups receiving locomotor training had a higher frequency of dizziness or faintness during treatment (P=0.008). Among patients with severe walking impairment, multiple falls were more common in the group receiving early locomotor training than in the other two groups (P=0.02).
Conclusions: Locomotor training, including the use of body-weight support in stepping on a treadmill, was not shown to be superior to progressive exercise at home managed by a physical therapist. (Funded by the National Institute of Neurological Disorders and Stroke and the National Center for Medical Rehabilitation Research; LEAPS ClinicalTrials.gov number, NCT00243919.).
Figures
References
-
- Heart disease and stroke statistics — 2010 update. Dallas: American Heart Association; 2010.
-
- Jørgensen HS, Nakayama H, Raaschou HO, Olsen TS. Recovery of walking function in stroke patients: the Copenhagen Stroke Study. Arch Phys Med Rehabil. 1995;76:27–32. - PubMed
-
- Weerdesteyn V, de Niet M, van Duijnhoven HJR, Geurts ACH. Falls in individuals with stroke. J Rehabil Res Dev. 2008;45:1195–213. - PubMed
-
- Pouwels S, Lalmohamed A, Leufkens B, et al. Risk of hip/femur fracture after stroke: a population-based case-control study. Stroke. 2009;40:3281–5. - PubMed
-
- Michael KM, Allen JK, Macko RF. Reduced ambulatory activity after stroke: the role of balance, gait, and cardiovascular fitness. Arch Phys Med Rehabil. 2005;86:1552–6. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials