

Subgroup analyses on return to work in sick-listed employees with low back pain in a randomised trial comparing brief and multidisciplinary intervention
- PMID: 21612625
- PMCID: PMC3121658
- DOI: 10.1186/1471-2474-12-112
Subgroup analyses on return to work in sick-listed employees with low back pain in a randomised trial comparing brief and multidisciplinary intervention
Abstract
Background: Multidisciplinary intervention is recommended for rehabilitation of employees sick-listed for 4-12 weeks due to low back pain (LBP). However, comparison of a brief and a multidisciplinary intervention in a randomised comparative trial of sick-listed employees showed similar return to work (RTW) rates in the two groups. The aim of the present study was to identify subgroups, primarily defined by work-related baseline factors that would benefit more from the multidisciplinary intervention than from the brief intervention.
Methods: A total of 351 employees sick-listed for 3-16 weeks due to LBP were recruited from their general practitioners. They received a brief or a multidisciplinary intervention. Both interventions comprised clinical examination and advice by a rehabilitation doctor and a physiotherapist. The multidisciplinary intervention also comprised assignment of a case manager, who made a rehabilitation plan in collaboration with the patient and a multidisciplinary team. Using data from a national database, we defined RTW as no sickness compensation benefit disbursement for four consecutive weeks within the first year after the intervention. At the first interview in the clinic, it was ensured that sick leave was primarily due to low back problems.Questionnaires were used to obtain data on health, disability, demographic and workplace-related factors. Cox hazard regression analyses were used with RTW as outcome measure and hazard rate ratios (HRR = HRmultidisciplinary/HRbrief) were adjusted for demographic and health-related variables. An interaction term consisting of a baseline variable*intervention group was added to the multivariable regression model to analyse whether the effects of the interventions were moderated by the baseline factor. Subsequently, a new study was performed that included 120 patients who followed the same protocol. This group was analyzed in the same way to verify the findings from the original study group.
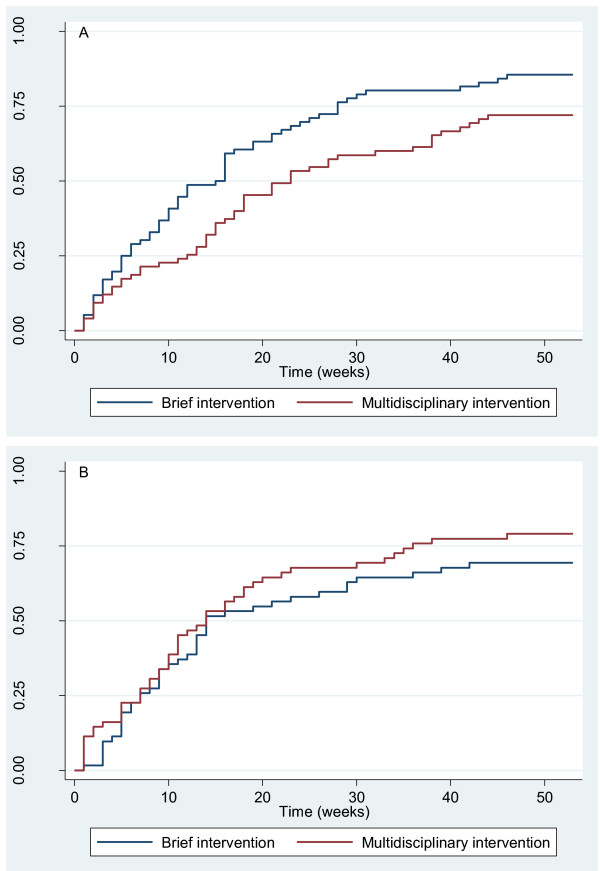
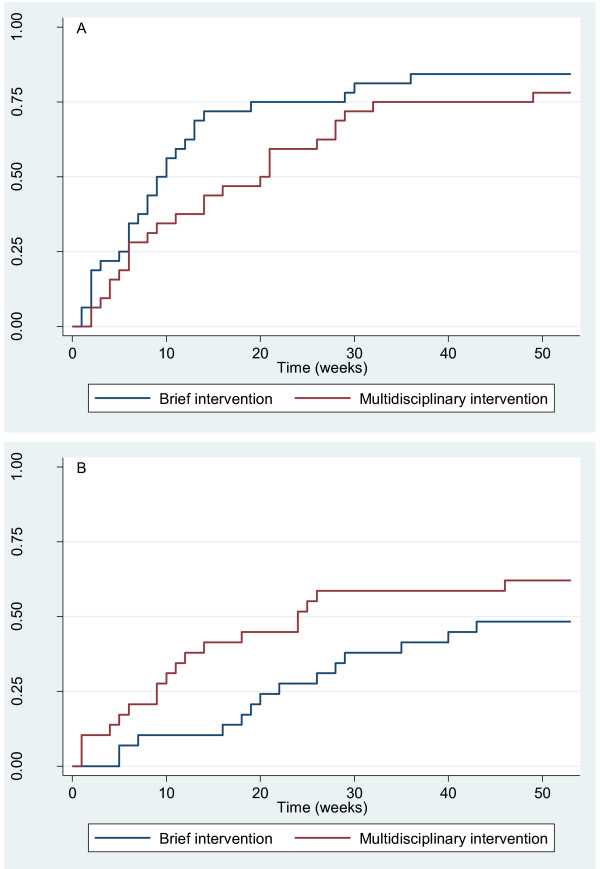
Results: The multidisciplinary intervention group ensured a quicker RTW than the brief intervention group in a subgroup with low job satisfaction, notably when claimants were excluded. The opposite effect was seen in the subgroup with high job satisfaction. When claimants were excluded, the effect was also in favour of the multidisciplinary intervention in subgroups characterised by no influence on work planning and groups at risk of losing their job. Inversely, the effect was in favour of the brief intervention in the subgroups who were able to influence the planning of their work and who had no risk of losing their job due to current sick leave. Interaction analysis of the data in the new study displayed similar or even more pronounced differences between subgroups in relation to intervention type.
Conclusions: Multidisciplinary intervention seemed more effective than brief intervention in subgroups of patients with low job satisfaction, no influence on work planning and feeling at risk of losing their jobs due to their sick leave as compared with subgroups not fulfilling these criteria.
Figures
Comment in
-
The impact of a brief vs. multidisciplinary intervention on return to work remains unclear for employees sick-listed with low back pain.Aust Occup Ther J. 2012 Jun;59(3):249-50. doi: 10.1111/j.1440-1630.2012.01020.x. Aust Occup Ther J. 2012. PMID: 22690777 No abstract available.
References
-
- Kjøller M, Juel K, Kamper-Jørgensen F. The Public Health Report Denmark 2007. Copenhagen, The National Institute of Public Health (SIF), University of Southern Denmark; 2007. pp. 1–482.
-
- Waddell G. The back pain revolution. 2. Elsevier Limited; 2004.
-
- Karjalainen K, Malmivaara A, van TM, Roine R, Jauhiainen M, Hurri H. et al.Multidisciplinary biopsychosocial rehabilitation for subacute low back pain in working-age adults: a systematic review within the framework of the Cochrane Collaboration Back Review Group. Spine (Phila Pa 1976) 2001;26:262–269. doi: 10.1097/00007632-200102010-00011. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Miscellaneous
