

Methylenetetrahydrofolate reductase (MTHFR) polymorphism A1298C (Glu429Ala) predicts decline in renal function over time in the African-American Study of Kidney Disease and Hypertension (AASK) Trial and Veterans Affairs Hypertension Cohort (VAHC)
- PMID: 21613384
- PMCID: PMC3350339
- DOI: 10.1093/ndt/gfr257
Methylenetetrahydrofolate reductase (MTHFR) polymorphism A1298C (Glu429Ala) predicts decline in renal function over time in the African-American Study of Kidney Disease and Hypertension (AASK) Trial and Veterans Affairs Hypertension Cohort (VAHC)
Abstract
Background: Hyperhomocysteinemia is associated with increased venous thrombosis and cardiovascular disease (CVD). Mutations in the human methylenetetrahydrofolate reductase (MTHFR) gene have been associated with increased homocysteine levels and risks of CVD in various populations including those with kidney disease. Here, we evaluated the influence of MTHFR variants on progressive loss of kidney function.
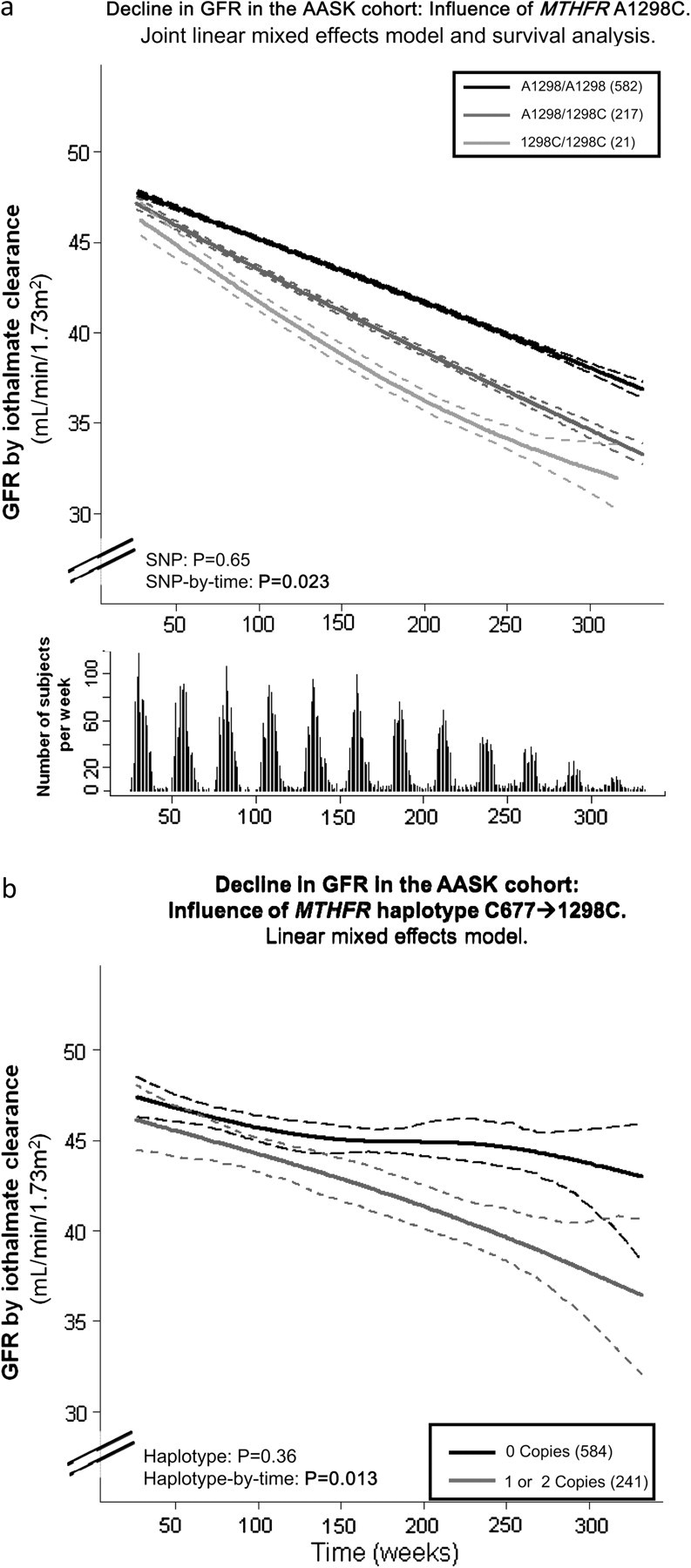
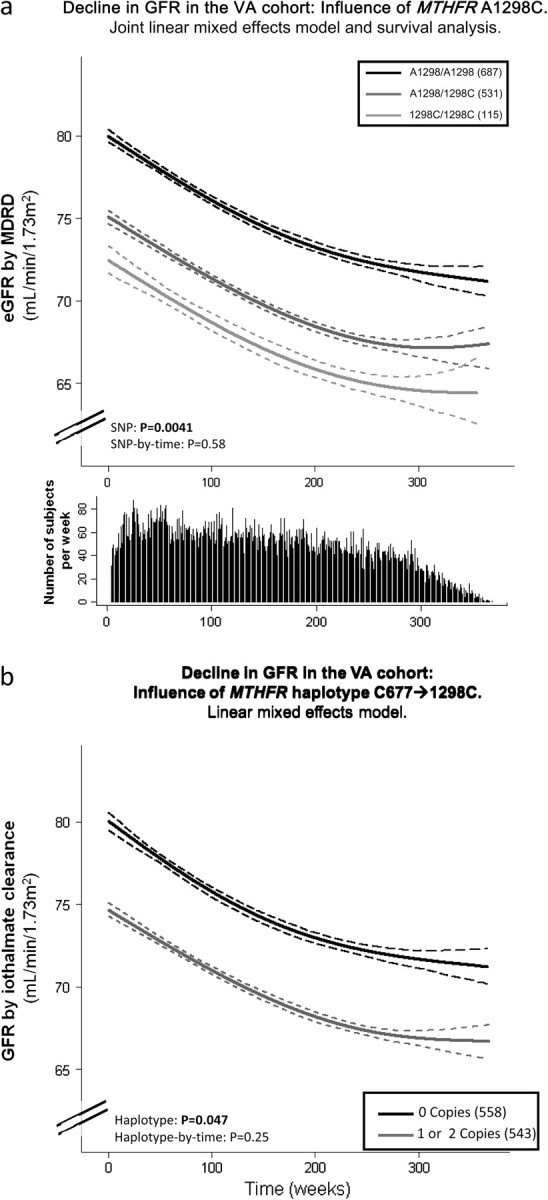
Methods: We analyzed 821 subjects with hypertensive nephrosclerosis from the longitudinal National Institute of Diabetes and Digestive and Kidney Diseases African-American Study of Kidney Disease and Hypertension (AASK) Trial to determine whether decline in glomerular filtration rate (GFR) over ∼4.2 years was predicted by common genetic variation within MTHFR at non-synonymous positions C677T (Ala222Val) and A1298C (Glu429Ala) or by MTHFR haplotypes. The effect on GFR decline was then supported by a study of 1333 subjects from the San Diego Veterans Affairs Hypertension Cohort (VAHC), followed over ∼4.5 years. Linear effect models were utilized to determine both genotype [single-nucleotide polymorphism (SNP)] and genotype (SNP)-by-time interactions.
Results: In AASK, the polymorphism at A1298C predicted the rate of GFR decline: A1298/A1298 major allele homozygosity resulted in a less pronounced decline of GFR, with a significant SNP-by-time interaction. An independent follow-up study in the San Diego VAHC subjects supports that A1298/A1298 homozygotes have the greatest estimated GFR throughout the study. Haplotype analysis with C677T yielded concurring results.
Conclusion: We conclude that the MTHFR-coding polymorphism at A1298C is associated with renal decline in African-Americans with hypertensive nephrosclerosis and is supported by a veteran cohort with a primary care diagnosis of hypertension. Further investigation is needed to confirm such findings and to determine what molecular mechanism may contribute to this association.
Figures
Similar articles
-
Adrenergic beta-1 receptor genetic variation predicts longitudinal rate of GFR decline in hypertensive nephrosclerosis.Nephrol Dial Transplant. 2009 Dec;24(12):3677-86. doi: 10.1093/ndt/gfp471. Epub 2009 Sep 10. Nephrol Dial Transplant. 2009. PMID: 19745105 Free PMC article.
-
The common mutations C677T and A1298C in the human methylenetetrahydrofolate reductase gene are associated with hyperhomocysteinemia and cardiovascular disease in hemodialysis patients.Nephron. 2002 Sep;92(1):120-6. doi: 10.1159/000064485. Nephron. 2002. PMID: 12187094
-
Association of MTHFR C677T and A1298C variants with preeclampsia risk and angiogenic imbalance in Tunisian women.Pregnancy Hypertens. 2025 Mar;39:101187. doi: 10.1016/j.preghy.2025.101187. Epub 2025 Jan 9. Pregnancy Hypertens. 2025. PMID: 39793459
-
Association of maternal and fetal MTHFR A1298C polymorphism with the risk of pregnancy loss: a study of an Indian population and a meta-analysis.Fertil Steril. 2013 Apr;99(5):1311-1318.e4. doi: 10.1016/j.fertnstert.2012.12.027. Epub 2013 Jan 26. Fertil Steril. 2013. PMID: 23357458
-
Relationship between methylenetetrahydrofolate reductase (MTHFR) gene (A1298C) polymorphism with the risk of stroke: A systematic review and meta-analysis.Neurol Res. 2020 Nov;42(11):913-922. doi: 10.1080/01616412.2020.1798107. Epub 2020 Jul 29. Neurol Res. 2020. PMID: 32727306
Cited by
-
Identifying multiple causative genes at a single GWAS locus.Genome Res. 2013 Dec;23(12):1996-2002. doi: 10.1101/gr.160283.113. Epub 2013 Sep 4. Genome Res. 2013. PMID: 24006081 Free PMC article.
-
Regression methods for investigating risk factors of chronic kidney disease outcomes: the state of the art.BMC Nephrol. 2014 Mar 14;15:45. doi: 10.1186/1471-2369-15-45. BMC Nephrol. 2014. PMID: 24628838 Free PMC article. Review.
-
The association between chronic renal failure and renal cell carcinoma may differ between black and white Americans.Cancer Causes Control. 2013 Jan;24(1):167-74. doi: 10.1007/s10552-012-0102-z. Epub 2012 Nov 21. Cancer Causes Control. 2013. PMID: 23179659 Free PMC article.
-
No association of the MTHFR gene A1298C polymorphism with the risk of prostate cancer: A meta-analysis.Exp Ther Med. 2012 Mar;3(3):493-498. doi: 10.3892/etm.2012.445. Epub 2012 Jan 4. Exp Ther Med. 2012. PMID: 22969917 Free PMC article.
-
Target organ damage in African American hypertension: role of APOL1.Curr Hypertens Rep. 2012 Feb;14(1):21-8. doi: 10.1007/s11906-011-0237-4. Curr Hypertens Rep. 2012. PMID: 22068337 Free PMC article. Review.
References
-
- van der Put NM, Steegers-Theunissen RP, Frosst P, et al. Mutated methylenetetrahydrofolate reductase as a risk factor for spina bifida. Lancet. 1995;346:1070–1071. - PubMed
-
- Den Heijer M, Lewington S, Clarke R. Homocysteine, MTHFR and risk of venous thrombosis: a meta-analysis of published epidemiological studies. J Thromb Haemost. 2005;3:292–299. - PubMed
-
- Homocysteine Studies Collaboration. Homocysteine and risk of ischemic heart disease and stroke: a meta-analysis. JAMA. 2002;288:2015–2022. - PubMed
-
- Boushey CJ, Beresford SA, Omenn GS, et al. A quantitative assessment of plasma homocysteine as a risk factor for vascular disease. Probable benefits of increasing folic acid intakes. JAMA. 1995;274:1049–1057. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- MD000220/MD/NIMHD NIH HHS/United States
- U01 DK048689/DK/NIDDK NIH HHS/United States
- M01 RR000071/RR/NCRR NIH HHS/United States
- T32 GM008666/GM/NIGMS NIH HHS/United States
- DK057867/DK/NIDDK NIH HHS/United States
- P60 MD000220/MD/NIMHD NIH HHS/United States
- RR00827/RR/NCRR NIH HHS/United States
- HL58120/HL/NHLBI NIH HHS/United States
- R01 DK057867/DK/NIDDK NIH HHS/United States
- U54 RR0252204-01/RR/NCRR NIH HHS/United States
- P01 HL058120/HL/NHLBI NIH HHS/United States
- M01 RR000827/RR/NCRR NIH HHS/United States
- RR000071/RR/NCRR NIH HHS/United States
- DK048689/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
