

Association of echocardiographic abnormalities with mortality in men with non-dialysis-dependent chronic kidney disease
- PMID: 21613387
- PMCID: PMC3350343
- DOI: 10.1093/ndt/gfr282
Association of echocardiographic abnormalities with mortality in men with non-dialysis-dependent chronic kidney disease
Abstract
Background: The interrelationship of left ventricular hypertrophy (LVH) with ejection fraction (EF) and their impact on mortality in non-dialysis-dependent chronic kidney disease (NDD-CKD) is unclear.
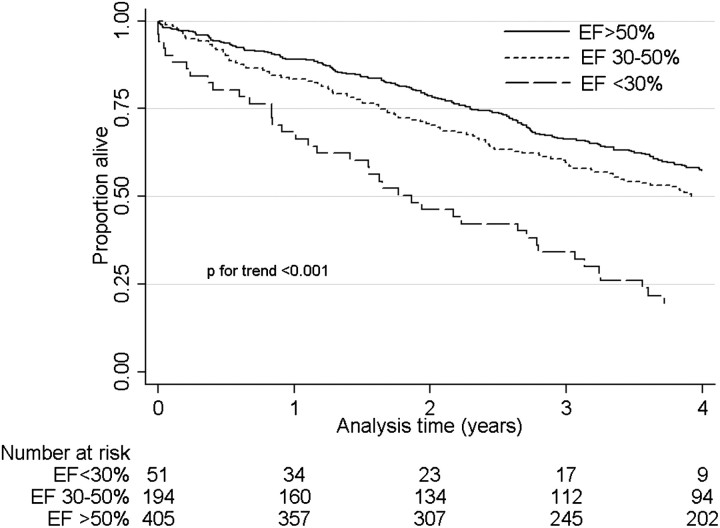
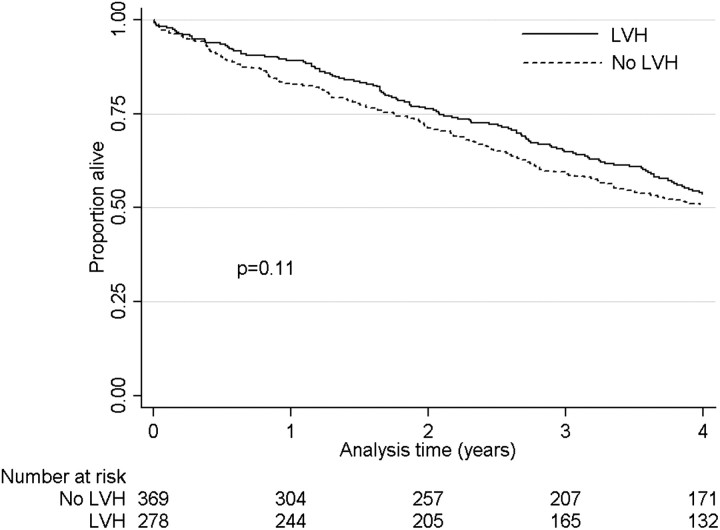
Methods: We examined the associations of EF and LVH with all-cause mortality in a historic cohort of 650 male US veterans with moderate-to-advanced NDD-CKD. EF and LVH were examined both separately and after categorizing patients according to their concomitant EF and presence/absence of LVH. Associations with mortality were examined in Cox models with adjustments for demographics, blood pressure, comorbidities, smoking status, medication use and biochemical characteristics.
Results: EF <30 and 30-50% were associated with higher all-cause mortality compared to EF >50% even after multivariable adjustments [multivariable adjusted hazard ratio, 95% confidence interval (CI): 2.83 (1.86-4.30) and 1.38 (1.06-1.78), P < 0.001 for linear trend]. LVH in itself was not associated with mortality [multivariable adjusted hazard ratio, 95% CI: 0.83 (0.66-1.05), P = 0.12], but the presence of LVH combined with an EF <50% was associated with the highest mortality [multivariable adjusted hazard ratios, 95% CI in patients with EF >50% + LVH, EF ≤ 50%-LVH and EF ≤ 50% + LVH, compared to EF >50%-LVH: 0.84 (0.63-1.13), 1.36 (1.00-1.83) and 1.62 (1.07-2.46)].
Conclusions: Low EF is associated with higher mortality in patients with NDD-CKD. In the presence of a low EF, LVH is also associated with higher mortality. Clinical trials are needed to determine if interventions targeting patients with low EF and LVH can lower mortality in NDD-CKD.
Figures
References
-
- Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am J Kidney Dis. 1998;32:S112–S119. - PubMed
-
- Garg AX, Clark WF, Haynes RB, et al. Moderate renal insufficiency and the risk of cardiovascular mortality: results from the NHANES I. Kidney Int. 2002;61:1486–1494. - PubMed
-
- Tonelli M, Wiebe N, Culleton B, et al. Chronic kidney disease and mortality risk: a systematic review. J Am Soc Nephrol. 2006;17:2034–2047. - PubMed
-
- Go AS, Chertow GM, Fan D, et al. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–1305. - PubMed
-
- Foley RN, Parfrey PS, Harnett JD, et al. Clinical and echocardiographic disease in patients starting end-stage renal disease therapy. Kidney Int. 1995;47:186–192. - PubMed
