

Keratinocyte apoptosis in epidermal remodeling and clearance of psoriasis induced by UV radiation
- PMID: 21614017
- PMCID: PMC3160491
- DOI: 10.1038/jid.2011.134
Keratinocyte apoptosis in epidermal remodeling and clearance of psoriasis induced by UV radiation
Abstract
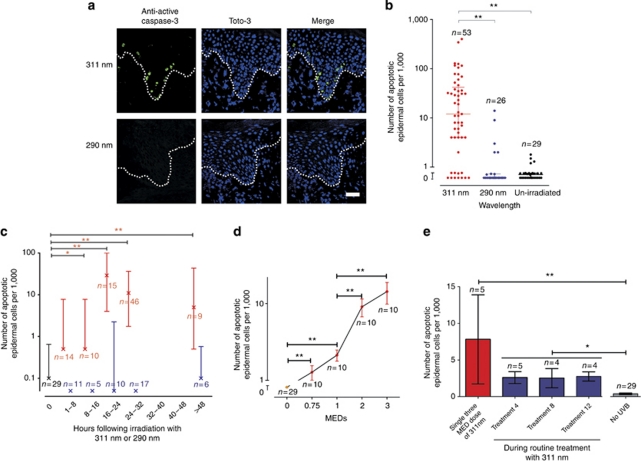
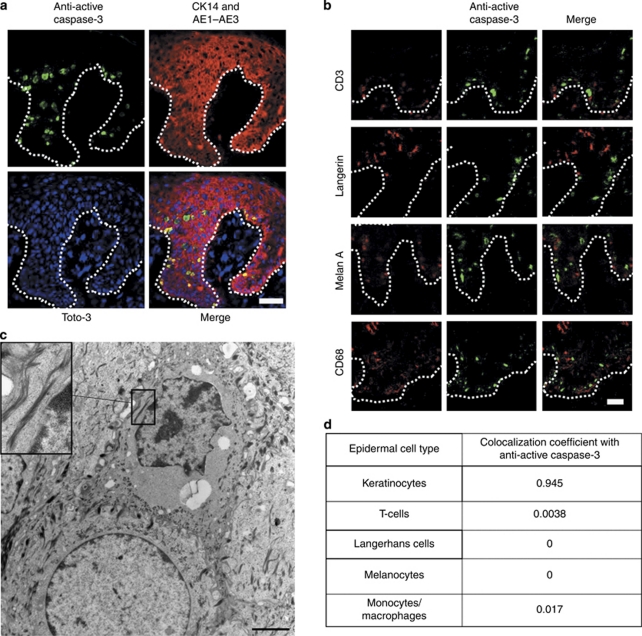
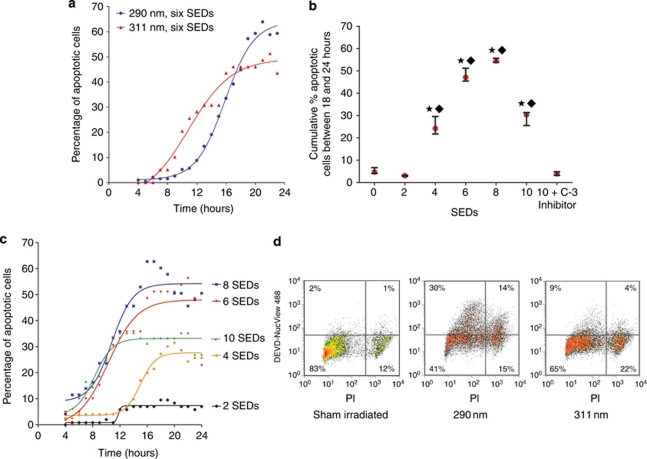
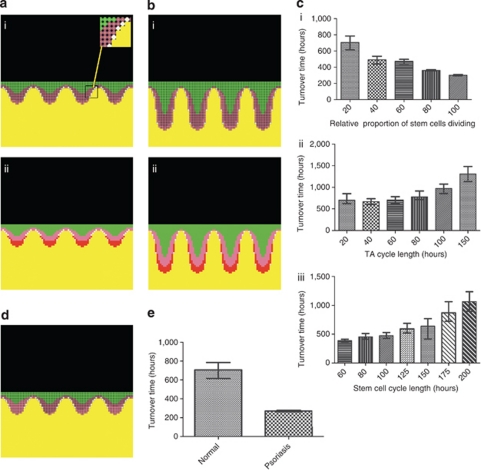
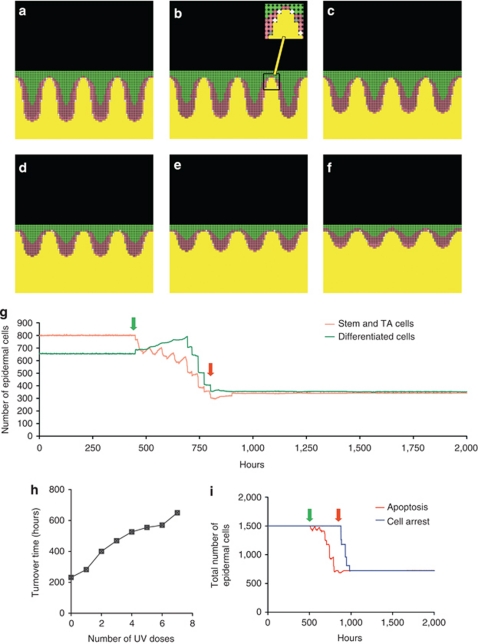
Psoriasis is a common chronic skin disorder, but the mechanisms involved in the resolution and clearance of plaques remain poorly defined. We investigated the mechanism of action of UVB, which is highly effective in clearing psoriasis and inducing remission, and tested the hypothesis that apoptosis is a key mechanism. To distinguish bystander effects, equal erythemal doses of two UVB wavelengths were compared following in vivo irradiation of psoriatic plaques; one is clinically effective (311 nm) and one has no therapeutic effect on psoriasis (290 nm). Only 311 nm UVB induced significant apoptosis in lesional epidermis, and most apoptotic cells were keratinocytes. To determine clinical relevance, we created a computational model of psoriatic epidermis. Modeling predicted apoptosis would occur in both stem and transit-amplifying cells to account for plaque clearance; this was confirmed and quantified experimentally. The median rate of keratinocyte apoptosis from onset to cell death was 20 minutes. These data were fed back into the model and demonstrated that the observed level of keratinocyte apoptosis was sufficient to explain UVB-induced plaque resolution. Our human studies combined with a systems biology approach demonstrate that keratinocyte apoptosis is a key mechanism in psoriatic plaques clearance, providing the basis for future molecular investigation and therapeutic development.
Figures
References
-
- Asawanonda P, Anderson RR, Chang Y, et al. 308-nm excimer laser for the treatment of psoriasis: a dose-response study. Arch Dermatol. 2000;136:619–624. - PubMed
-
- Cen H, Mao F, Aronchik I, et al. DEVD-NucView488: a novel class of enzyme substrates for real-time detection of caspase-3 activity in live cells. FASEB J. 2008;22:2243–2252. - PubMed
-
- Coven TR, Burack LH, Gilleaudeau R, et al. Narrowband UV-B produces superior clinical and histopathological resolution of moderate-to-severe psoriasis in patients compared with broadband UV-B. Arch Dermatol. 1997;133:1514–1522. - PubMed
-
- Dawe RS, Wainwright NJ, Cameron H, et al. Narrow-band (TL-01) ultraviolet B phototherapy for chronic plaque psoriasis: three times or five times weekly treatment. Br J Dermatol. 1998;138:833–839. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
