

A Review of Fetal ECG Signal Processing; Issues and Promising Directions
- PMID: 21614148
- PMCID: PMC3100207
- DOI: 10.2174/1876536X01003010004
A Review of Fetal ECG Signal Processing; Issues and Promising Directions
Abstract
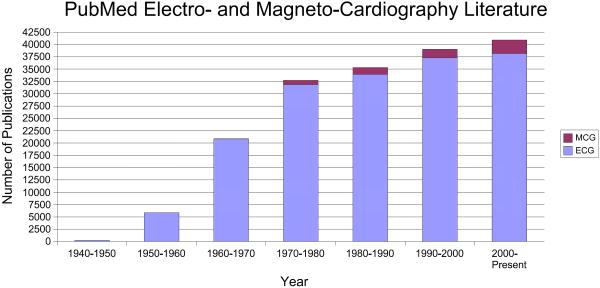
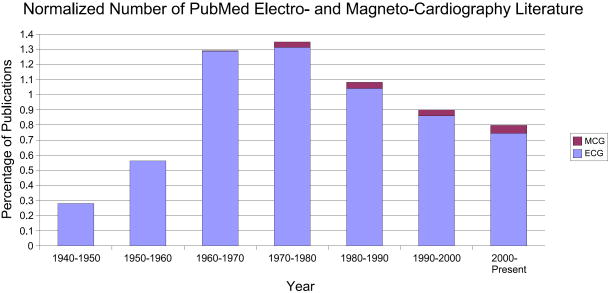
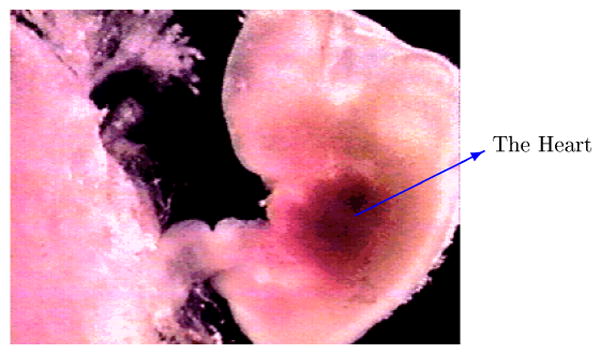
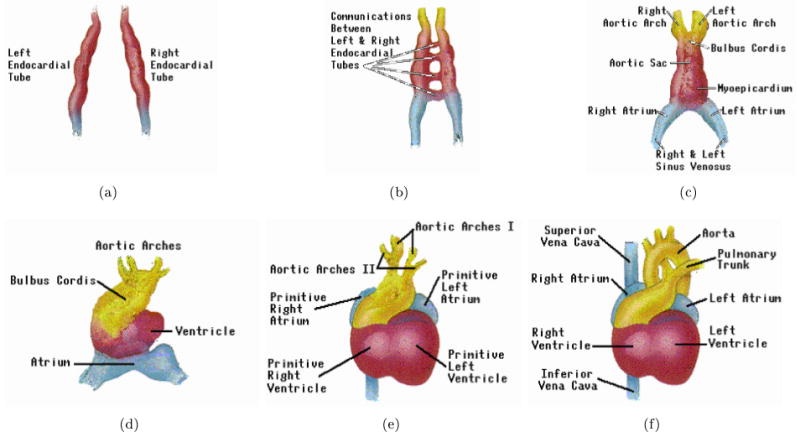
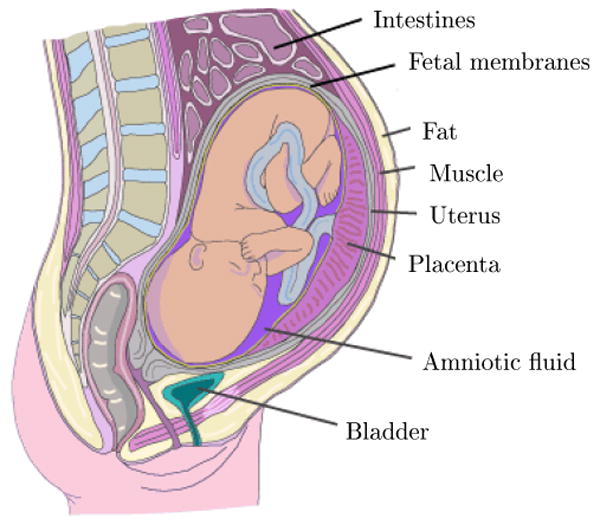
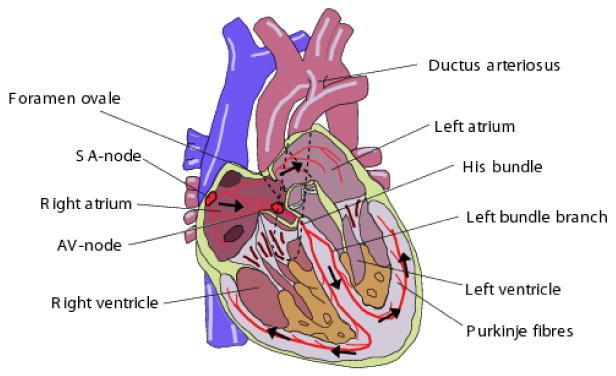
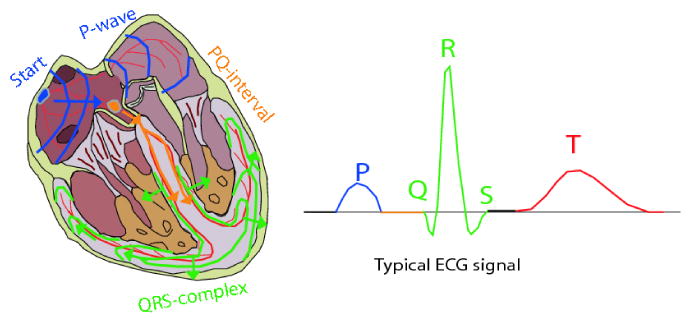
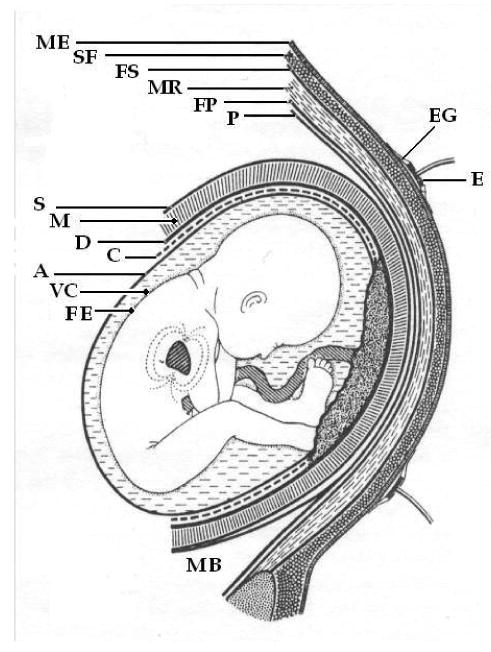
The field of electrocardiography has been in existence for over a century, yet despite significant advances in adult clinical electrocardiography, signal processing techniques and fast digital processors, the analysis of fetal ECGs is still in its infancy. This is, partly due to a lack of availability of gold standard databases, partly due to the relatively low signal-to-noise ratio of the fetal ECG compared to the maternal ECG (caused by the various media between the fetal heart and the measuring electrodes, and the fact that the fetal heart is simply smaller), and in part, due to the less complete clinical knowledge concerning fetal cardiac function and development. In this paper we review a range of promising recording and signal processing techniques for fetal ECG analysis that have been developed over the last forty years, and discuss both their shortcomings and advantages. Before doing so, however, we review fetal cardiac development, and the etiology of the fetal ECG. A selection of relevant models for the fetal/maternal ECG mixture is also discussed. In light of current understanding of the fetal ECG, we then attempt to justify recommendations for promising future directions in signal processing, and database creation.
Conflict of interest statement
Figures
References
-
- Congenital Heart Defects. March of Dimes. 2005. [Online]. Available: http://www.marchofdimes.com/professionals/14332_1212.asp.
-
- Minino AM, Heron MP, Murphy SL, Kochanek KD. Deaths: Final data for 2004. National Vital Statistics Reports. Aug, 2007. - PubMed
-
- Congenital Heart Defects in Children Fact Sheet. American Heart Association; 2008. [Online]. Available: http://www.americanheart.org/children.
-
- Pajkrt E, Weisz B, Firth HV, Chitty LS. Fetal cardiac anomalies and genetic syndromes. Prenat Diagn. Dec, 2004. pp. 1104–1115. [Online]. Available: http://dx.doi.org/10.1002/pd.1067. - DOI - PubMed
-
- Zuckerwar A, Pretlow R, Stoughton J, Baker D. Development of a piezopolymer pressure sensor for a portable fetal heart rate monitor. IEEE Trans Biomed Eng. 1993;40(no. 9):963–969. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources