

Medical management of paraquat ingestion
- PMID: 21615775
- PMCID: PMC3243009
- DOI: 10.1111/j.1365-2125.2011.04026.x
Medical management of paraquat ingestion
Abstract
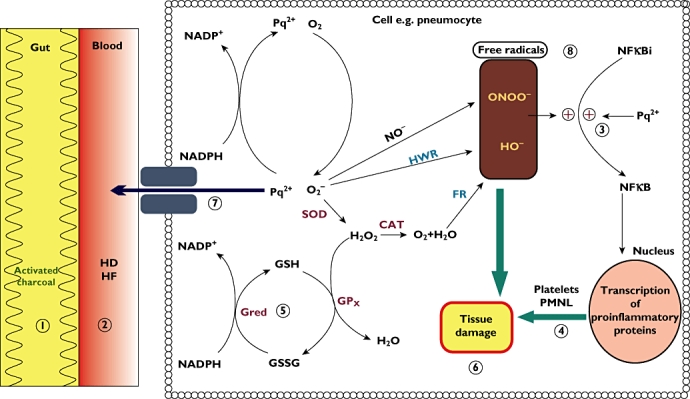
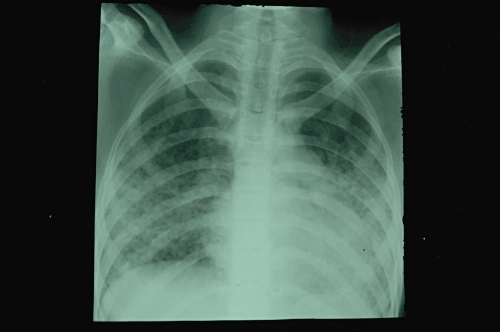
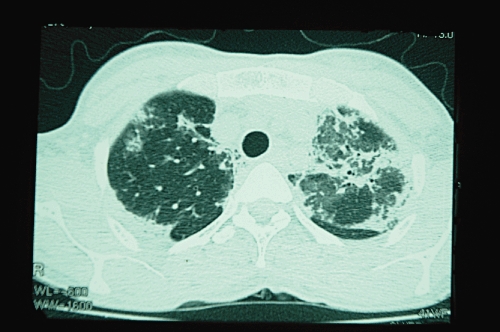
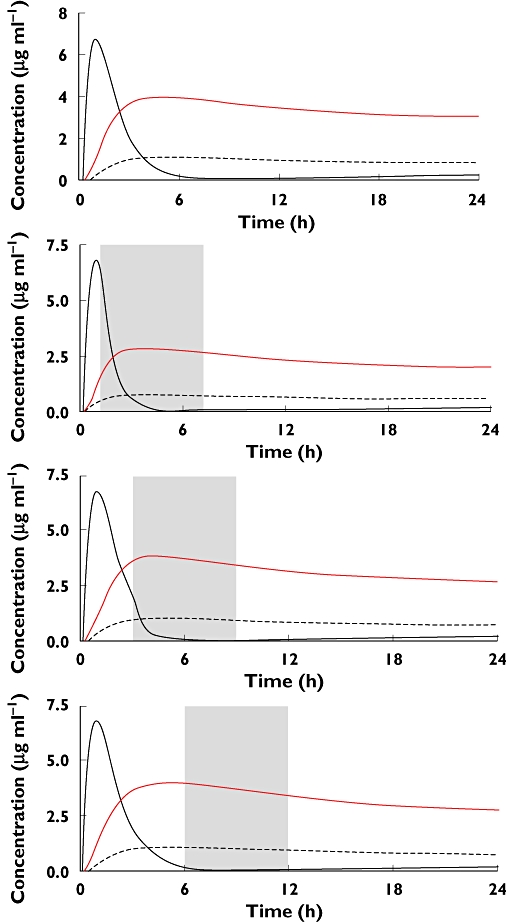
Poisoning by paraquat herbicide is a major medical problem in parts of Asia while sporadic cases occur elsewhere. The very high case fatality of paraquat is due to inherent toxicity and lack of effective treatments. We conducted a systematic search for human studies that report toxicokinetics, mechanisms, clinical features, prognosis and treatment. Paraquat is rapidly but incompletely absorbed and then largely eliminated unchanged in urine within 12-24 h. Clinical features are largely due to intracellular effects. Paraquat generates reactive oxygen species which cause cellular damage via lipid peroxidation, activation of NF-κB, mitochondrial damage and apoptosis in many organs. Kinetics of distribution into these target tissues can be described by a two-compartment model. Paraquat is actively taken up against a concentration gradient into lung tissue leading to pneumonitis and lung fibrosis. Paraquat also causes renal and liver injury. Plasma paraquat concentrations, urine and plasma dithionite tests and clinical features provide a good guide to prognosis. Activated charcoal and Fuller's earth are routinely given to minimize further absorption. Gastric lavage should not be performed. Elimination methods such as haemodialysis and haemoperfusion are unlikely to change the clinical course. Immunosuppression with dexamethasone, cyclophosphamide and methylprednisolone is widely practised, but evidence for efficacy is very weak. Antioxidants such as acetylcysteine and salicylate might be beneficial through free radical scavenging, anti-inflammatory and NF-κB inhibitory actions. However, there are no published human trials. The case fatality is very high in all centres despite large variations in treatment.
© 2011 The Authors. British Journal of Clinical Pharmacology © 2011 The British Pharmacological Society.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
