

Mild-to-moderate hypothermia in aortic arch surgery using circulatory arrest: a change of paradigm?
- PMID: 21616675
- PMCID: PMC3241078
- DOI: 10.1016/j.ejcts.2011.03.060
Mild-to-moderate hypothermia in aortic arch surgery using circulatory arrest: a change of paradigm?
Abstract
Objectives: Antegrade cerebral perfusion makes deep hypothermia non-essential for neuroprotection; therefore, there is a growing tendency to increase the body temperature during circulatory arrest with selective brain perfusion. However, very little is known about the clinical efficacy of mild-to-moderate hypothermia for ischemic organ protection during circulatory arrest. The aim of this study was to evaluate the safety and efficiency of mild-to-moderate hypothermia for lower-body protection during aortic arch surgery with circulatory arrest and antegrade cerebral perfusion.
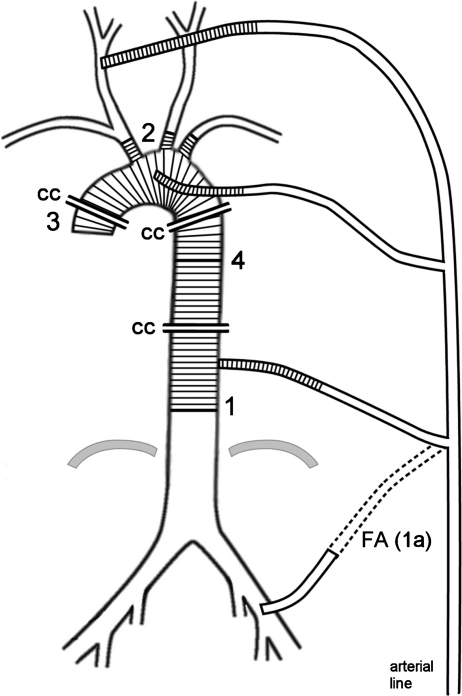
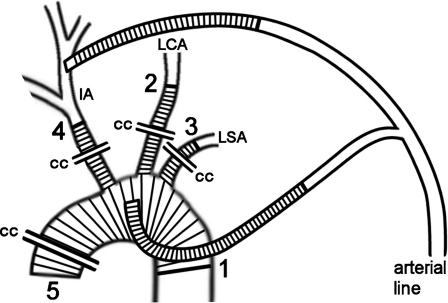
Methods: Between January 2005 and December 2009, a total of 347 patients underwent non-emergent arch surgery. In all patients, the systematic cooling was adapted to the expected time of circulatory arrest, and cerebral perfusion was performed at a constant blood temperature of 28 °C. There were 40 cardiac or aortic re-operations, 312 patients had concomitant aortic valve or root surgery, and 10 patients had replacement of the descending aorta. All examined data were collected prospectively.
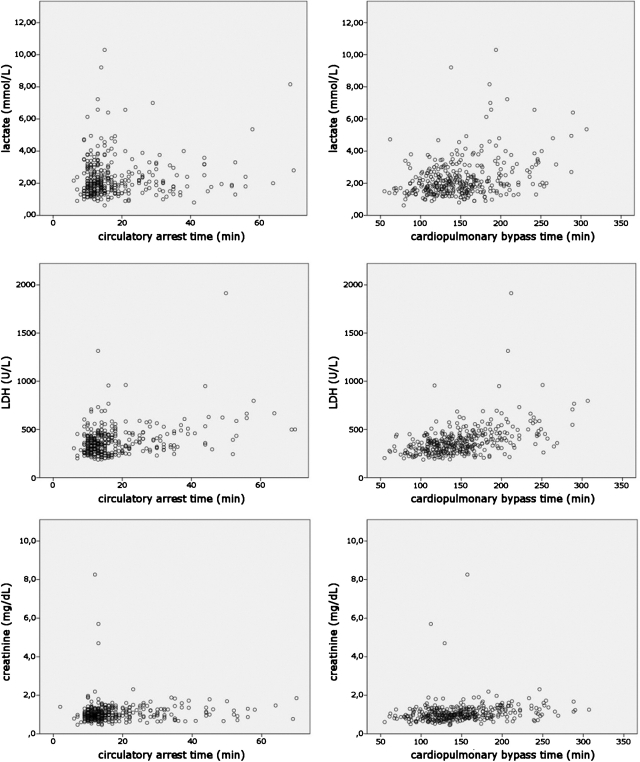
Results: The duration of circulatory arrest and the deepest rectal temperature were 18±11 min (range, 6-70 min) and 31.5±1.6 °C (range, 26.0-35.0 °C) for all 347 patients, and 34±12 min (range, 17-70 min) and 29.9±1.7 °C (range, 26.0-34.6 °C) for 77 patients having total/subtotal arch replacement. The maximum serum lactate level on the first postoperative day was, on average, 2.3±1.2 mmol l(-1). In the statistical analysis, no association between the duration of temperature-adapted circulatory arrest and lactate, creatinine, or lactate dehydrogenase levels after surgery could be demonstrated. The 30-day mortality was 0.9%. Permanent neurological deficit or temporary dysfunction occurred in three (0.9%) and eight (2.3%) patients, respectively. No paraplegia and no hepatic failure were reported; however, mesenteric ischemia occurred in one patient with severe stenosis of the celiac and upper mesenteric arteries. Temporary dialysis was necessary primarily after surgery in five patients. All of them underwent hemiarch replacement only, and four patients had an increased creatinine level before surgery.
Conclusion: Systemic mild-to-moderate hypothermia that is adapted to the duration of circulatory arrest is a simple, safe, and effective method of organ protection and can be recommended in routine aortic arch surgery with circulatory arrest and cerebral perfusion.
Figures
Comment in
-
A paradigm shift in aortic arch surgery, certainly--but corroboration required.Eur J Cardiothorac Surg. 2012 Jan;41(1):191-2. doi: 10.1016/j.ejcts.2011.05.003. Eur J Cardiothorac Surg. 2012. PMID: 21704528 Free PMC article. No abstract available.
-
Aortic arch surgery with a mild-to-moderate circulatory arrest: the significance of aortic arch pathology.Eur J Cardiothorac Surg. 2012 Sep;42(3):602; author reply 602-3. doi: 10.1093/ejcts/ezs161. Epub 2012 Apr 4. Eur J Cardiothorac Surg. 2012. PMID: 22491669 No abstract available.
-
Extended mild hypothermic aortic surgery.Eur J Cardiothorac Surg. 2013 Jan;43(1):205. doi: 10.1093/ejcts/ezs317. Epub 2012 May 31. Eur J Cardiothorac Surg. 2013. PMID: 22653448 No abstract available.
References
-
- Kirklin J, Barrat-Boyes B. Hypothermia, circulatory arrest, and cardiopulmonary bypass. In: Kirklin J, Barrat-Boyes, editors. Cardiac surgery. Philadelphia: Churchill-Livingstone; 2003. pp. 66–130.
-
- Urbanski PP, Lenos A, Blume JC, Ziegler V, Griewing B, Schmitt R, Diegeler A, Dinkel M. Does anatomical completeness of the circle of Willis correlate with sufficient cross-perfusion during unilateral cerebral perfusion? Eur J Cardiothorac Surg. 2008;33:402–8. - PubMed
-
- Urbanski PP. Cannulation of the left common carotid artery for proximal aortic repair. J Thorac Cardiovasc Surg. 2003;126:887–8. - PubMed
-
- Urbanski PP, Lenos A, Lindemann Y, Weigang E, Zacher M, Diegeler A. Carotid artery cannulation in aortic surgery. J Thorac Cardiovasc Surg. 2006;132:1398–403. - PubMed
-
- Urbanski PP, Lenos A, Lindemann Y, Zacher M, Frank S, Diegeler A. Use of a carotid artery for arterial cannulation: side-related differences. Thorac Cardiovasc Surg. 2010;58:276–9. - PubMed
