

Calcific aortic valve stenosis: methods, models, and mechanisms
- PMID: 21617136
- PMCID: PMC3150727
- DOI: 10.1161/CIRCRESAHA.110.234138
Calcific aortic valve stenosis: methods, models, and mechanisms
Abstract
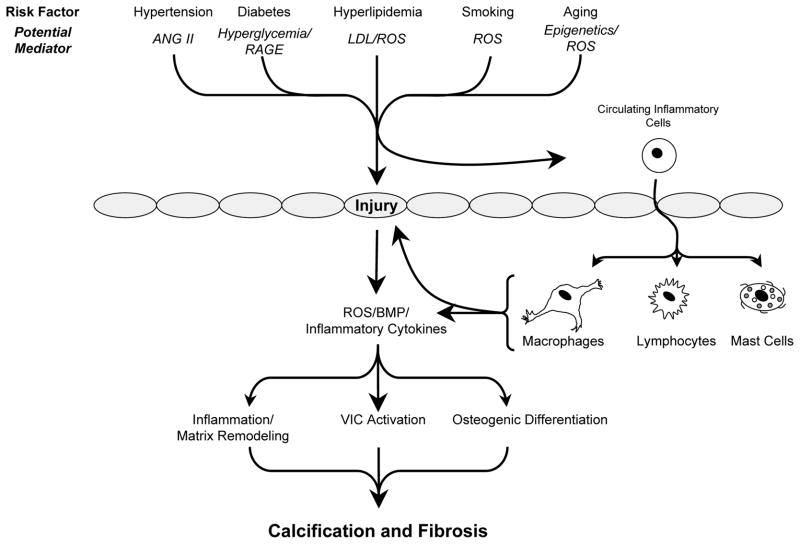
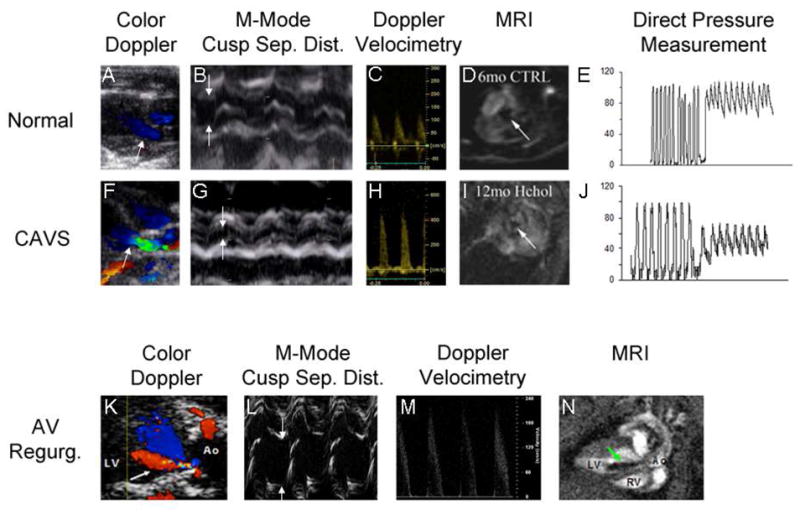
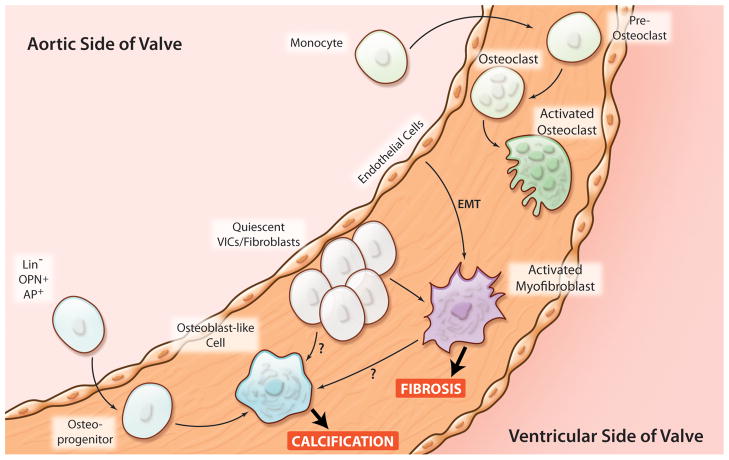
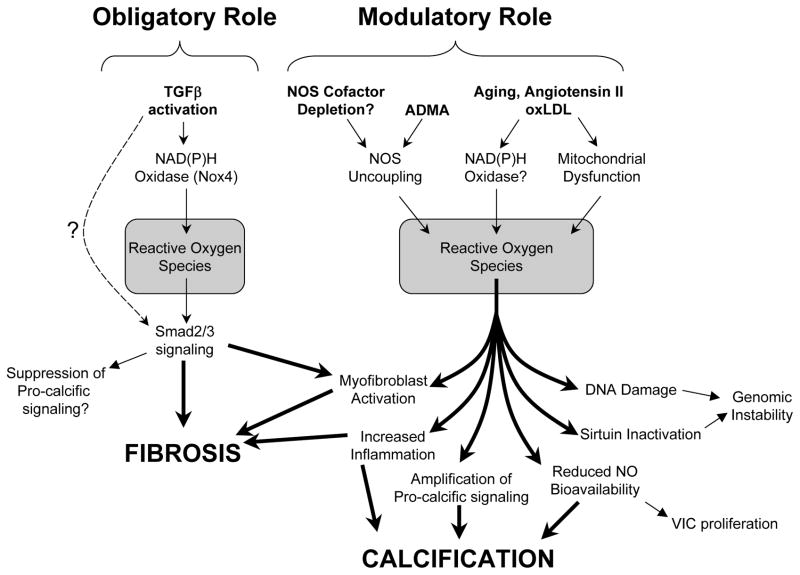
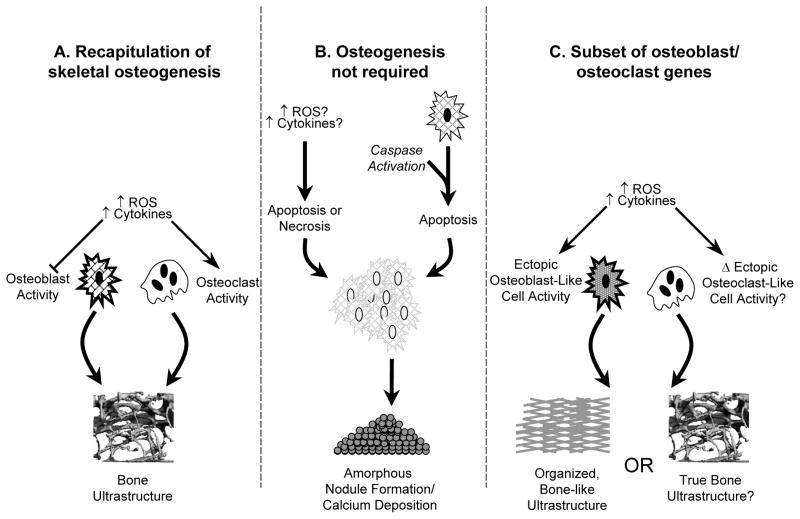
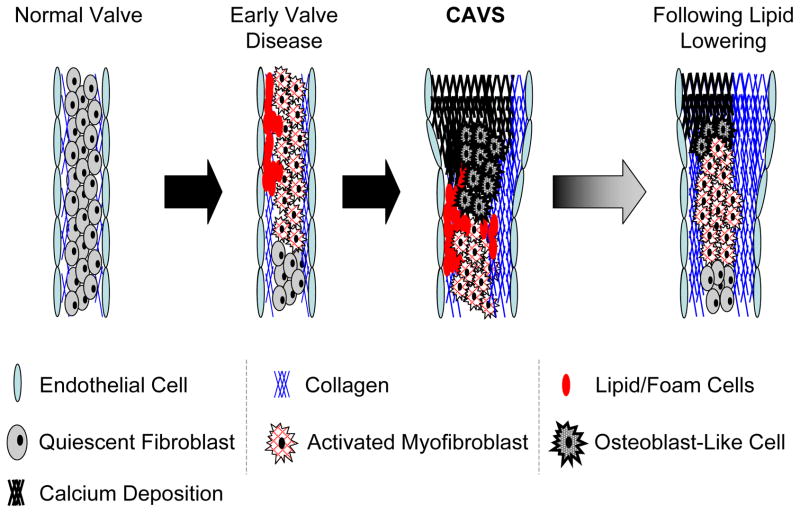
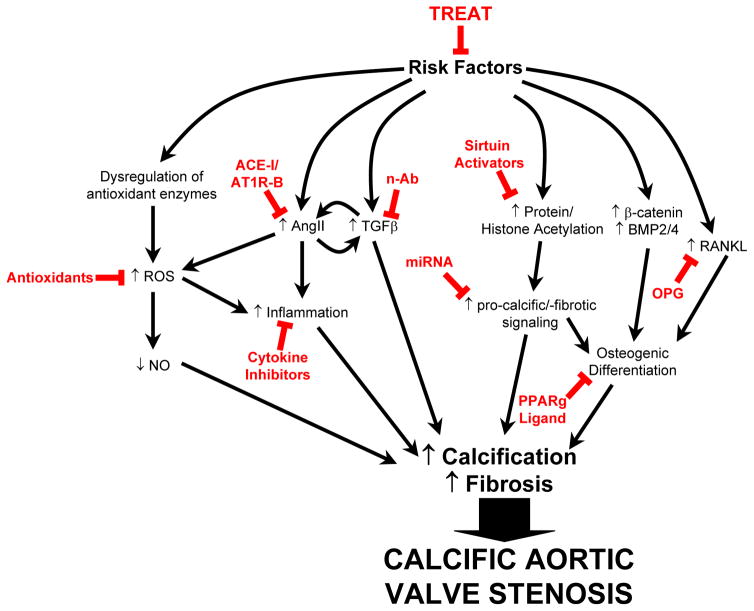
Calcific aortic valve stenosis (CAVS) is a major health problem facing aging societies. The identification of osteoblast-like and osteoclast-like cells in human tissue has led to a major paradigm shift in the field. CAVS was thought to be a passive, degenerative process, whereas now the progression of calcification in CAVS is considered to be actively regulated. Mechanistic studies examining the contributions of true ectopic osteogenesis, nonosseous calcification, and ectopic osteoblast-like cells (that appear to function differently from skeletal osteoblasts) to valvular dysfunction have been facilitated by the development of mouse models of CAVS. Recent studies also suggest that valvular fibrosis, as well as calcification, may play an important role in restricting cusp movement, and CAVS may be more appropriately viewed as a fibrocalcific disease. High-resolution echocardiography and magnetic resonance imaging have emerged as useful tools for testing the efficacy of pharmacological and genetic interventions in vivo. Key studies in humans and animals are reviewed that have shaped current paradigms in the field of CAVS, and suggest promising future areas for research.
Conflict of interest statement
Two of the authors (DDH and RMW) have received osteoprotegerin, and a research grant, from Amgen, Inc.
Figures
References
-
- Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: A population-based study. Lancet. 2006;368:1005–1011. - PubMed
-
- Bonow RO, Carabello BA, Chatterjee K, de Leon AC, Jr, Faxon DP, Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O’Gara PT, O’Rourke RA, Otto CM, Shah PM, Shanewise JS. 2008 focused update incorporated into the acc/aha 2006 guidelines for the management of patients with valvular heart disease: A report of the american college of cardiology/american heart association task force on practice guidelines (writing committee to revise the 1998 guidelines for the management of patients with valvular heart disease): Endorsed by the society of cardiovascular anesthesiologists, society for cardiovascular angiography and interventions, and society of thoracic surgeons. Circulation. 2008;118:e523–661. - PubMed
-
- Messika-Zeitoun D, Bielak LF, Peyser PA, Sheedy PF, Turner ST, Nkomo VT, Breen JF, Maalouf J, Scott C, Tajik AJ, Enriquez-Sarano M. Aortic valve calcification: Determinants and progression in the population. Arterioscler Thromb Vasc Biol. 2007;27:642–648. - PubMed
-
- Freeman RV, Otto CM. Spectrum of calcific aortic valve disease: Pathogenesis, disease progression, and treatment strategies. Circulation. 2005;111:3316–3326. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
