

Aging causes collateral rarefaction and increased severity of ischemic injury in multiple tissues
- PMID: 21617137
- PMCID: PMC3141082
- DOI: 10.1161/ATVBAHA.111.227314
Aging causes collateral rarefaction and increased severity of ischemic injury in multiple tissues
Abstract
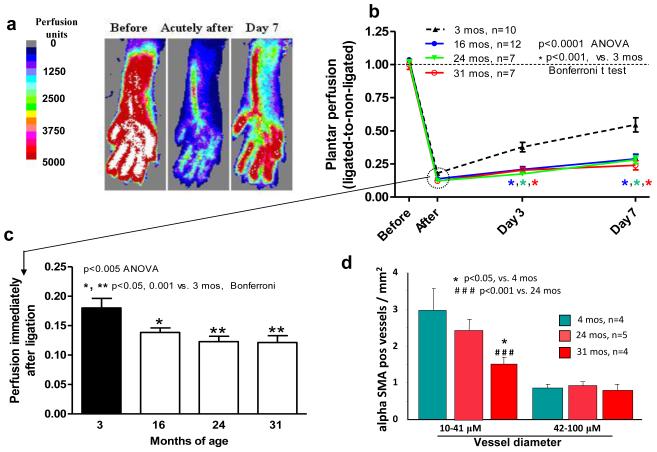
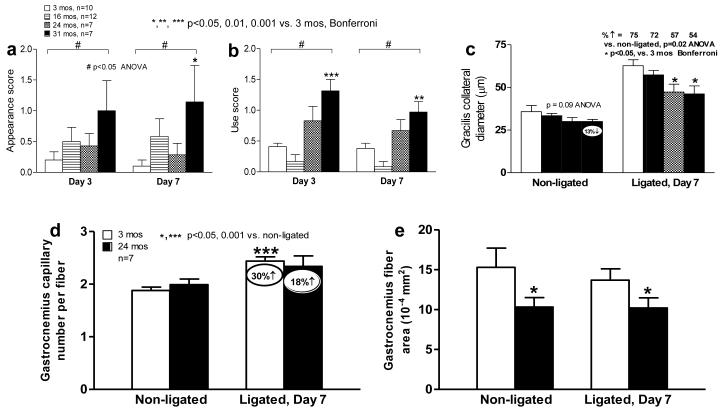
Objective: Aging is a major risk factor for increased ischemic tissue injury. Whether collateral rarefaction and impaired remodeling contribute to this is unknown. We quantified the number and diameter of native collaterals and their remodeling in 3-, 16-, 24-, and 31-month-old mice.
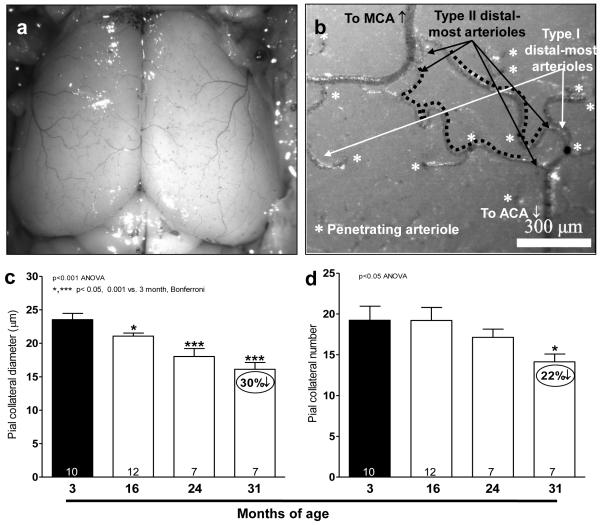
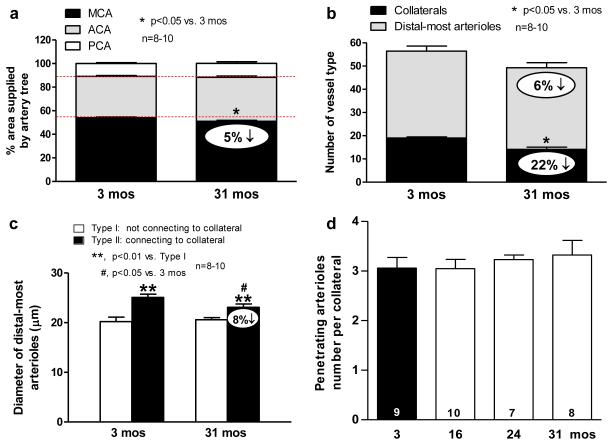
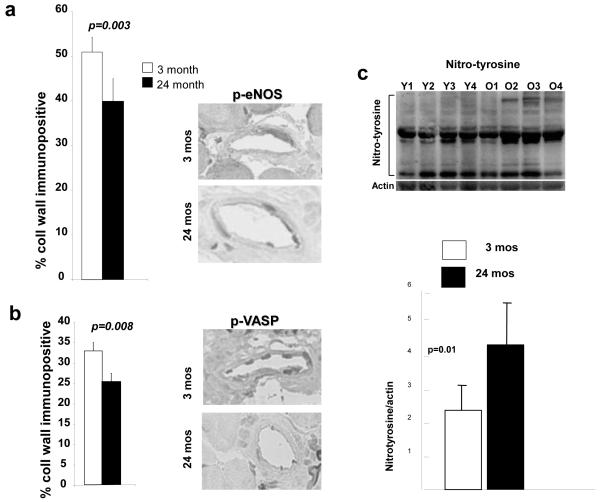
Methods and results: Aging caused an "age-dose-dependent" greater drop in perfusion immediately after femoral artery ligation, followed by a diminished recovery of flow and increase in tissue injury. These effects were associated with a decline in collateral number, diameter, and remodeling. Angiogenesis was also impaired. Mechanistically, these changes were not accompanied by reduced recruitment of T cells or macrophages to remodeling collaterals. However, endothelial nitric oxide synthase signaling was dysfunctional, as indicated by increased protein nitrosylation and less phosphorylated endothelial nitric oxide synthase and vasodilator-stimulated phosphoprotein in collateral wall cells. The cerebral circulation exhibited a similar age-dose-dependent loss of collateral number and diameter and increased tortuosity, resulting in an increase in collateral resistance and infarct volume (eg, 6- and 3-fold, respectively, in 24-month-old mice) after artery occlusion. This was not associated with rarefaction of similarly sized arterioles. Collateral remodeling was also reduced.
Conclusions: Our findings demonstrate that aging causes rarefaction and insufficiency of the collateral circulation in multiple tissues, resulting in more severe ischemic tissue injury.
Figures


References
-
- Cooper LT, Cooke JP, Dzau VJ. The vasculopathy of aging. J Gerontol. 1994;49:B191–196. - PubMed
-
- Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, De Simone G, Ferguson TB, Ford E, Furie K, Gillespie C, Go A, Greenlund K, Haase N, Hailpern S, Ho PM, Howard V, Kissela B, Kittner S, Lackland D, Lisabeth L, Marelli A, McDermott MM, Meigs J, Mozaffarian D, Mussolino M, Nichol G, Roger VL, Rosamond W, Sacco R, Sorlie P, Stafford R, Thom T, Wasserthiel-Smoller S, Wong ND, Wylie-Rosett J. Heart disease and stroke statistics--2010 update: a report from the American Heart Association. Circulation. 2010;121:e46–e215. - PubMed
-
- Pedelty L, Gorelick PB. Management of hypertension and cerebrovascular disease in the elderly. Am J Med. 2008;121(8 Suppl):S23–31. - PubMed
-
- Ohta T, Hosaka M, Ishibashi H, Sugimoto I, Mihara E, Hida K, Takeuchi N, Hachiya J, Kato M, Kazui H, Nagata Y. Limb salvage and survival rates among elderly patients with advanced limb ischemia. Surg Today. 1998;28:156–61. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
