

Emergence of parapneumonic empyema in the USA
- PMID: 21617169
- PMCID: PMC4820002
- DOI: 10.1136/thx.2010.156406
Emergence of parapneumonic empyema in the USA
Abstract
Background: Although recent reports suggest that the incidence of parapneumonic empyema has increased in several regions of the USA, national trends in disease burden are unknown. National trends in the incidence of parapneumonic empyema hospitalisations and changes in empyema by associated pathogens were examined.
Methods: National hospitalisation data (1996-2008) were analysed and rates estimated using census estimates as denominators. Incidence rate ratios (IRR) compared 2008 with 1996 rates. Discharge diagnosis codes were used to characterise pathogens associated with empyema hospitalisations.
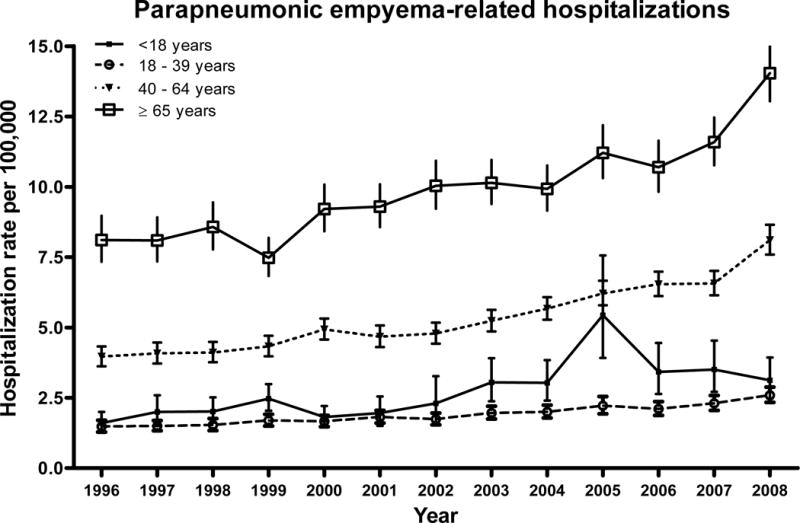
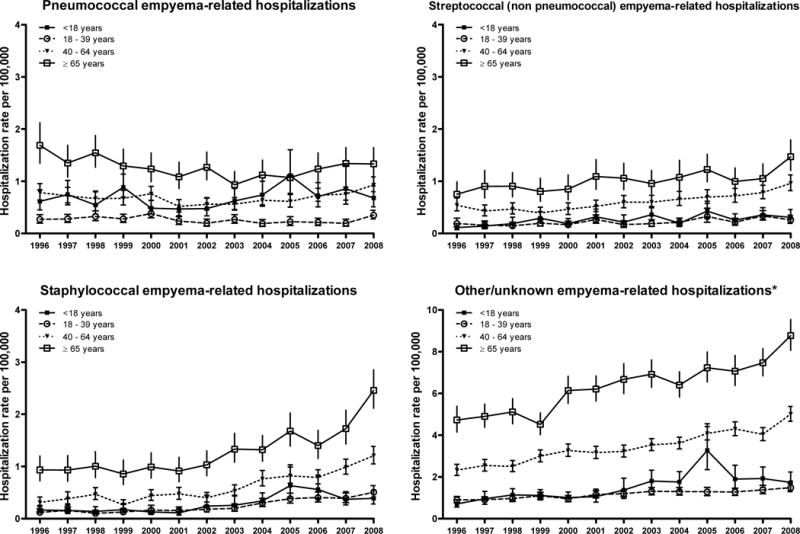
Results: Overall, national parapneumonic empyema-related hospitalisation rates increased from 3.04 per 100,000 in 1996 to 5.98 per 100,000 in 2008, a 2.0-fold increase (95% CI 1.8 to 2.1). The increases were observed among children (IRR 1.9 (95% CI 1.4 to 2.7)) and adults aged 18-39, 40-64 and ≥65 years (IRR 1.8 (95% CI 1.5 to 2.1), 2.0 (95% CI 1.6 to 3.1) and 1.7 (95% CI 1.5 to 2.0), respectively). Overall, pneumococcal empyema rates remained relatively stable in all age groups whereas streptococcal- (non-pneumococcal) and staphylococcal-related empyema rates increased 1.9-fold and 3.3-fold, respectively, with consistent increases across age groups. The overall in-hospital case fatality ratio for parapneumonic empyema-related hospitalisations was 8.0% (95% CI 6.4% to 9.5%) in 1996 and 7.2% (95% CI 6.3% to 8.1%) in 2008 (p=0.395). Of the empyemas where study pathogens were listed (37.6%), staphylococcal-related empyema had the largest absolute increases across age groups and was associated with longer hospital stay and higher in-hospital mortality than other empyemas.
Conclusions: Although parapneumonic empyema-related hospitalisations remained relatively rare, they increased substantially during the study period. A number of pathogens, especially staphylococcus, contributed to this increase.
Conflict of interest statement
Figures
Comment in
-
Pleural infection on the increase but with a better evidence base to inform clinical care.Thorax. 2011 Aug;66(8):649-50. doi: 10.1136/thx.2011.161315. Epub 2011 Jun 15. Thorax. 2011. PMID: 21680570 No abstract available.
References
-
- Septimus E. Pleural Effusion and Empyema. In: Mandell GL, Bennett JERD, editors. Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. Edinburgh: Churchill Livingstone; 2009. pp. 917–924. An imprint of ELSEVIER.
-
- Ashbaugh DG. Empyema thoracis. Factors influencing morbidity and mortality. Chest. 1991 May;99(5):1162–1165. - PubMed
-
- Ahmed RA, Marrie TJ, Huang JQ. Thoracic empyema in patients with community-acquired pneumonia. Am J Med. 2006 Oct;119(10):877–883. - PubMed
-
- Li ST, Gates RL. Primary operative management for pediatric empyema: decreases in hospital length of stay and charges in a national sample. Arch Pediatr Adolesc Med. 2008 Jan;162(1):44–48. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical