

Subcutaneous abatacept versus intravenous abatacept: a phase IIIb noninferiority study in patients with an inadequate response to methotrexate
- PMID: 21618201
- PMCID: PMC3229984
- DOI: 10.1002/art.30463
Subcutaneous abatacept versus intravenous abatacept: a phase IIIb noninferiority study in patients with an inadequate response to methotrexate
Abstract
Objective: To compare the efficacy and safety of subcutaneous (SC) and intravenous (IV) abatacept.
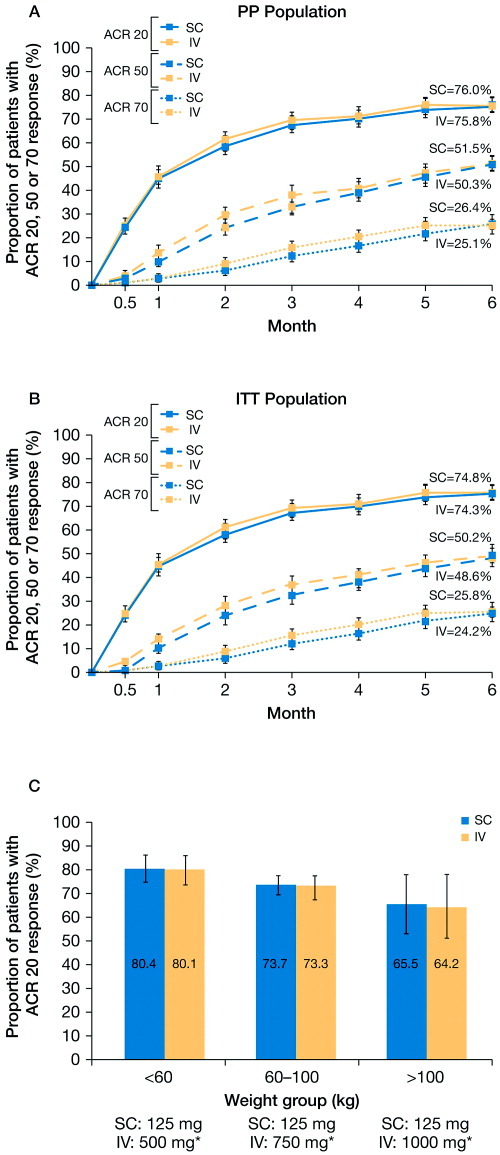
Methods: In this phase IIIb double-blind, double-dummy, 6-month study, patients with rheumatoid arthritis (RA) and inadequate responses to methotrexate were randomized to receive 125 mg SC abatacept on days 1 and 8 and weekly thereafter (plus an IV loading dose [∼10 mg/kg] on day 1) or IV abatacept (∼10 mg/kg) on days 1, 15, and 29 and every 4 weeks thereafter. The primary end point for determining the noninferiority of SC abatacept to IV abatacept was the proportion of patients in each group meeting the American College of Rheumatology 20% improvement criteria (achieving an ACR20 response) at month 6. Other efficacy end points, immunogenicity, and safety were also assessed.
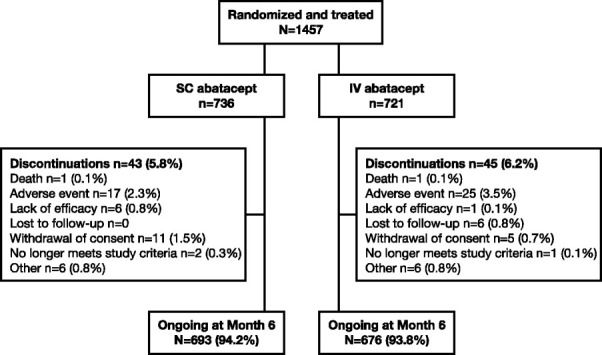
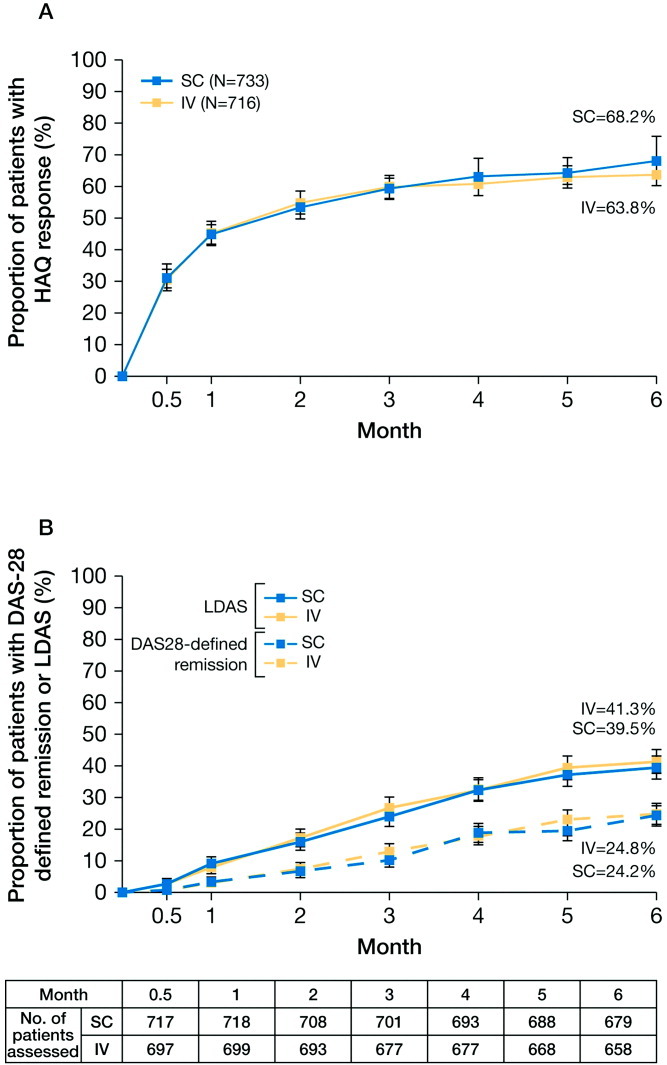
Results: Of 1,457 patients, 693 of 736 (94.2%) treated with SC abatacept and 676 of 721 (93.8%) treated with IV abatacept completed 6 months. At month 6, 76.0% (95% confidence interval 72.9, 79.2) of SC abatacept-treated patients versus 75.8% (95% confidence interval 72.6, 79.0) of IV abatacept-treated patients achieved an ACR20 response (estimated difference between groups 0.3% [95% confidence interval -4.2, 4.8]), confirming noninferiority of SC abatacept to IV abatacept. Onset and magnitude of ACR responses and disease activity and physical function improvements were comparable between the SC and IV abatacept-treated groups. The proportions of adverse events (AEs) and serious AEs over 6 months were 67.0% and 4.2%, respectively, in the SC abatacept-treated group and 65.2% and 4.9%, respectively, in the IV abatacept-treated group, with comparable frequencies of serious infections, malignancies, and autoimmune events between groups. SC injection site reactions (mostly mild) occurred in 19 SC abatacept (IV placebo)-treated patients (2.6%) and 18 IV abatacept (SC placebo)-treated patients (2.5%). Abatacept-induced antibodies occurred in 1.1% of SC abatacept-treated patients and 2.3% of IV abatacept-treated patients.
Conclusion: SC abatacept provides efficacy and safety comparable with that of IV abatacept, with low immunogenicity and high retention rates, consistent with the established IV abatacept profile. Rates of injection site reactions were low. SC abatacept will provide additional treatment options, such as an alternative route of administration, for patients with RA.
Trial registration: ClinicalTrials.gov NCT00559585.
Copyright © 2011 by the American College of Rheumatology.
Figures
Comment in
-
Dr. Genovese comments.J Rheumatol. 2015 Oct;42(10):1994. doi: 10.3899/jrheum.150600. J Rheumatol. 2015. PMID: 26429208 No abstract available.
References
-
- Bulpitt KJ. Biologic therapies in rheumatoid arthritis. Curr Rheumatol Rep. 1999;1:157–63. - PubMed
-
- Emery P, Durez P, Dougados M, Legerton CW, Becker JC, Vratsanos G, et al. Impact of T-cell costimulation modulation in patients with undifferentiated inflammatory arthritis or very early rheumatoid arthritis: a clinical and imaging study of abatacept (the ADJUST trial) Ann Rheum Dis. 2010;69:510–6. - PMC - PubMed
-
- Genovese MC, Becker JC, Schiff M, Luggen M, Sherrer Y, Kremer J, et al. Abatacept for rheumatoid arthritis refractory to tumor necrosis factor α inhibition. N Engl J Med. 2005;353:1114–23. - PubMed
-
- Genovese MC, Schiff M, Luggen M, Becker JC, Aranda R, Teng J, et al. Efficacy and safety of the selective co-stimulation modulator abatacept following 2 years of treatment in patients with rheumatoid arthritis and an inadequate response to anti-tumour necrosis factor therapy. Ann Rheum Dis. 2008;67:547–54. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
