

A prospective study of shoulder pain in primary care: prevalence of imaged pathology and response to guided diagnostic blocks
- PMID: 21619663
- PMCID: PMC3127806
- DOI: 10.1186/1471-2474-12-119
A prospective study of shoulder pain in primary care: prevalence of imaged pathology and response to guided diagnostic blocks
Abstract
Background: The prevalence of imaged pathology in primary care has received little attention and the relevance of identified pathology to symptoms remains unclear. This paper reports the prevalence of imaged pathology and the association between pathology and response to diagnostic blocks into the subacromial bursa (SAB), acromioclavicular joint (ACJ) and glenohumeral joint (GHJ).
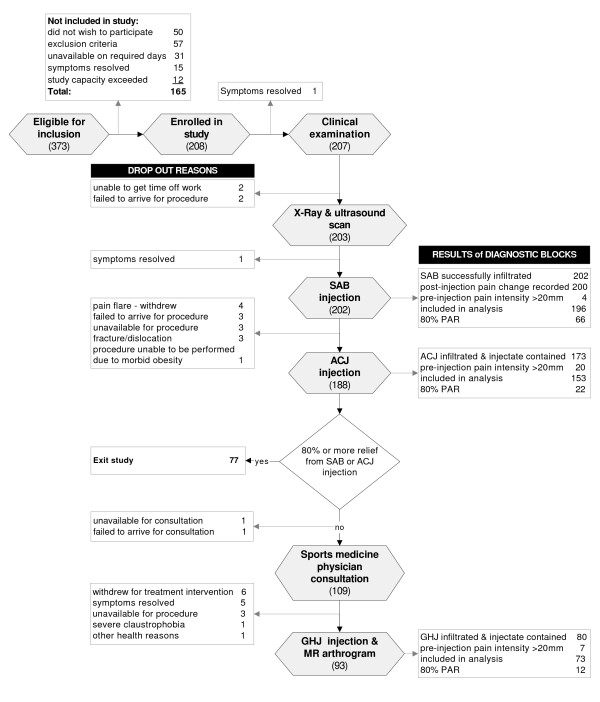
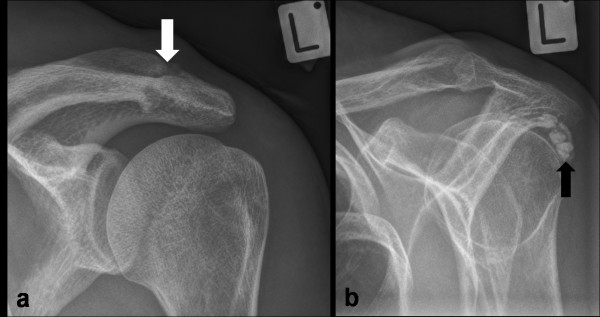
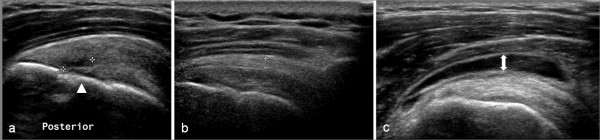
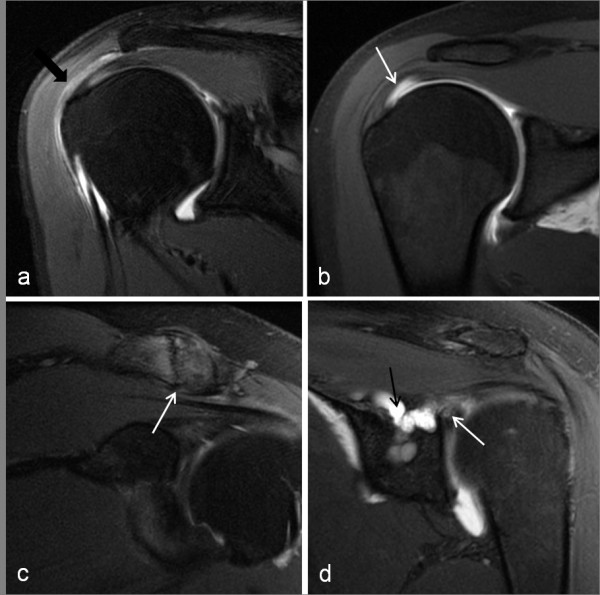
Methods: Consecutive patients with shoulder pain recruited from primary care underwent standardised x-ray, diagnostic ultrasound scan and diagnostic injections of local anaesthetic into the SAB and ACJ. Subjects who reported less than 80% reduction in pain following either of these injections were referred for a magnetic resonance arthrogram (MRA) and GHJ diagnostic block. Differences in proportions of positive and negative imaging findings in the anaesthetic response groups were assessed using Fishers test and odds ratios were calculated a for positive anaesthetic response (PAR) to diagnostic blocks.
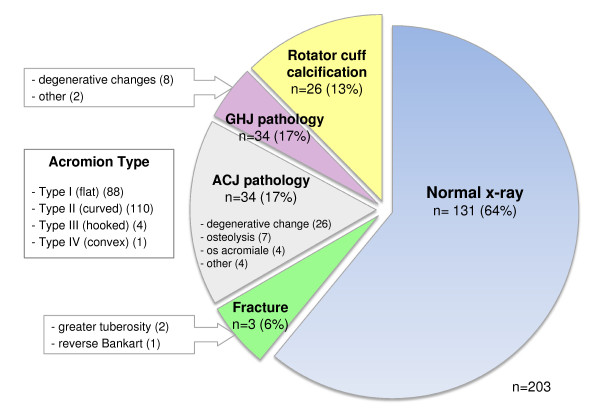
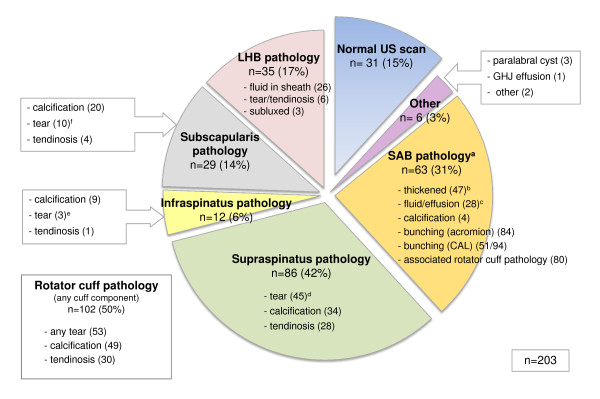
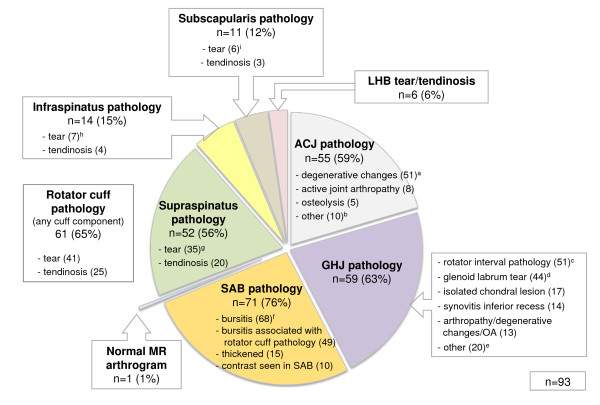
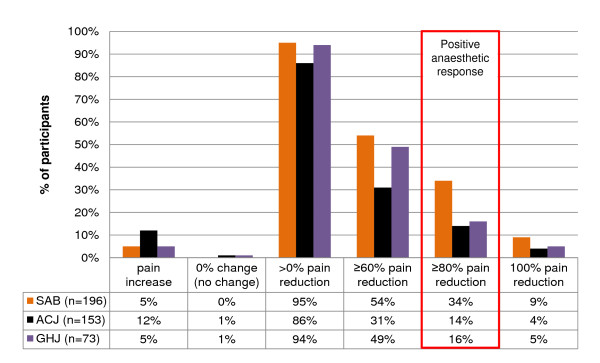
Results: In the 208 subjects recruited, the rotator cuff and SAB displayed the highest prevalence of pathology on both ultrasound (50% and 31% respectively) and MRA (65% and 76% respectively). The prevalence of PAR following SAB injection was 34% and ACJ injection 14%. Of the 59% reporting a negative anaesthetic response (NAR) for both of these injections, 16% demonstrated a PAR to GHJ injection. A full thickness tear of supraspinatus on ultrasound was associated with PAR to SAB injection (OR 5.02; p < 0.05). Ultrasound evidence of a biceps tendon sheath effusion (OR 8.0; p < 0.01) and an intact rotator cuff (OR 1.3; p < 0.05) were associated with PAR to GHJ injection. No imaging findings were strongly associated with PAR to ACJ injection (p ≤ 0.05).
Conclusions: Rotator cuff and SAB pathology were the most common findings on ultrasound and MRA. Evidence of a full thickness supraspinatus tear was associated with symptoms arising from the subacromial region, and a biceps tendon sheath effusion and an intact rotator cuff were associated with an intra-articular GHJ pain source. When combined with clinical information, these results may help guide diagnostic decision making in primary care.
Figures
References
-
- Urwin M, Symmons D, Allison T, Brammah T, Busby H, Roxby M, Simmons A, Williams G. Estimating the burden of musculoskeletal disorders in the community: the comparative prevalence of symptoms at different anatomical sites, and the relation to social deprivation. Ann Rheum Dis. 1998;57:649–655. doi: 10.1136/ard.57.11.649. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
