

Identifying suspected breast cancer: development and validation of a clinical prediction rule
- PMID: 21619744
- PMCID: PMC3080225
- DOI: 10.3399/bjgp11X572391
Identifying suspected breast cancer: development and validation of a clinical prediction rule
Abstract
Background: An evidence-based approach is needed to identify women with breast symptoms who are most likely to have breast cancer so that timely and appropriate referral can take place.
Aim: To report the development and validation of a clinical prediction rule for the diagnosis of breast cancer.
Design and setting: Cohort study with two prospective groups of women: those presenting to a symptomatic breast clinic (derivation cohort) and a separate cohort presenting to 11 general practices (validation cohort) in Tayside, Scotland.
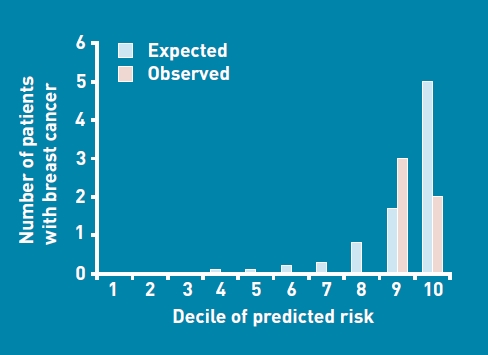
Method: Regression analysis was used to derive a clinical prediction rule from presenting symptoms, personal and family history, and clinical findings. Validation consisted of estimating the number of breast cancers predicted to occur compared with the actual number of observed breast cancers across deciles of risk.
Results: In the derivation cohort of 802 patients, 59 (7%) were diagnosed with breast cancer. Independent clinical predictors for breast cancer were: increasing age by year (adjusted odds ratio [AOR] 1.10, 95% confidence interval [CI] = 1.07 to 1.13); presence of a discrete lump (AOR 15.20, 95% CI = 4.88 to 47.34); breast thickening (AOR 7.64, 95% CI = 2.23 to 26.11); lymphadenopathy (AOR 3.63, 95% CI = 1.33 to 9.92); and lump ≥ 2 cm (AOR 5.41, 95% CI = 2.36 to 12.38). All eight patients with skin tethering had breast cancer. The regression model had good predictive power, identifying all five breast cancers in the validation cohort of 97 patients in the top two deciles of risk.
Conclusion: The clinical prediction rule discriminates between patients at high risk of breast cancer from those at low risk, and can be implemented as an evidence-based recommendation to enhance appropriate referral from general practice to a symptomatic breast clinic. Ongoing validation in further populations is required.
Figures
Comment in
-
Development and validation of a clinical prediction rule for breast cancer.Br J Gen Pract. 2011 Jun;61(587):382; author reply 382. doi: 10.3399/bjgp11X572661. Br J Gen Pract. 2011. PMID: 21801527 Free PMC article. No abstract available.
References
-
- Veronesi U, Boyle P, Goldhirsch A, et al. Breast cancer. Lancet. 2005;365(9472):1727–1741. - PubMed
-
- Newton P, Hannay DR, Laver R. The presentation and management of female breast symptoms in general practice in Sheffield. Fam Pract. 1999;16(4):360–365. - PubMed
-
- Roberts MM, Elton RA, Robinson SE, French K. Consultations for breast disease in general practice and hospital referral patterns. Br J Surg. 1987;74(11):1020–1022. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical