

Resident and fellow experiences after the introduction of endovascular aneurysm repair for abdominal aortic aneurysm
- PMID: 21620615
- PMCID: PMC4385217
- DOI: 10.1016/j.jvs.2011.03.008
Resident and fellow experiences after the introduction of endovascular aneurysm repair for abdominal aortic aneurysm
Abstract
Objectives: This study assessed trends in open and endovascular repair (EVAR) of intact and ruptured abdominal aortic aneurysm (AAA) in the Medicare population and evaluated recent trends in AAA repair at vascular fellowship training programs.
Methods: We identified all Medicare beneficiaries with a diagnosis of AAA who underwent repair or had a primary diagnosis of rupture (1995-2008). Cohorts were compared by type of repair (open vs EVAR) and presentation (intact vs ruptured AAA). Demographics of age, sex, and race were evaluated. We used unique hospital identifier codes to compare trends and 30-day mortality between hospitals that participate in vascular surgery fellowship training and those that do not. American Council on Graduate Medical Education data, only available for the years 1999 to 2008, were further used to better understand the changes in number of EVAR and open repairs of AAA performed each year for vascular fellows and general surgery residents, over time.
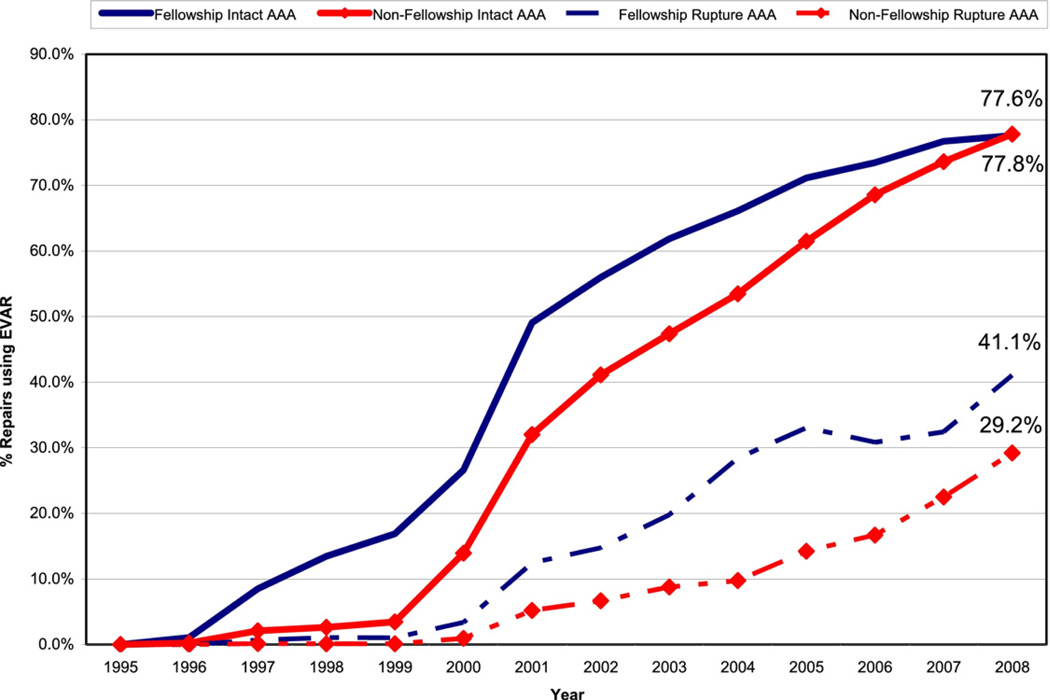
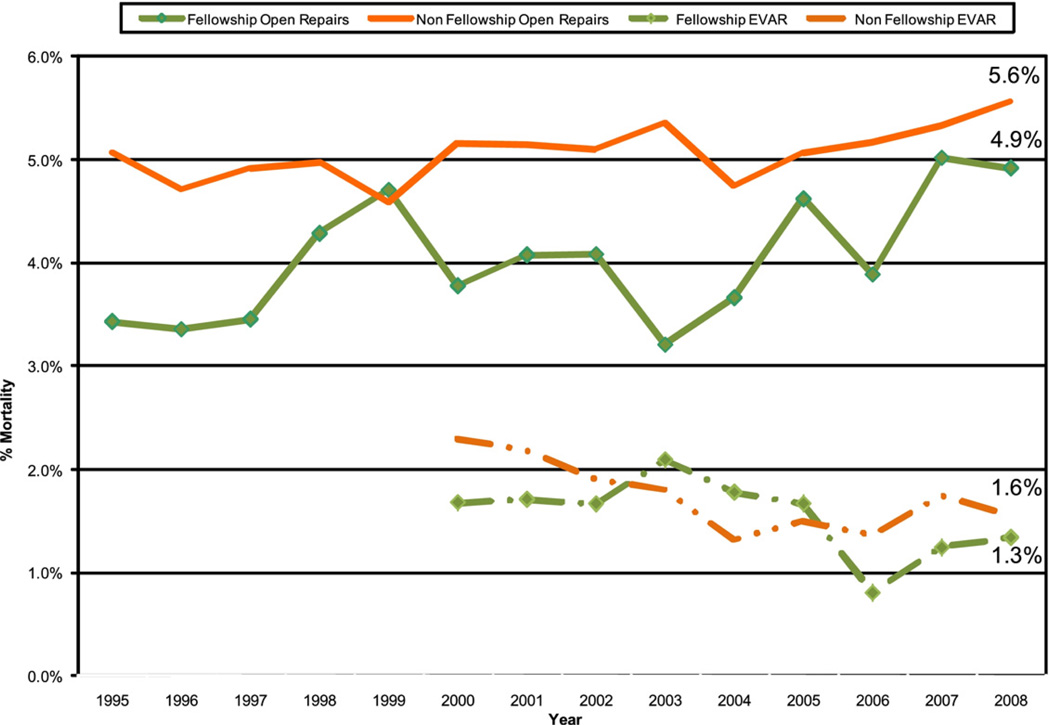
Results: We identified 449,122 patients (76% men), with 376,355 intact AAAs (84%) and 72,767 ruptured AAAs (16%). Mean age was 75.1 years. Use of EVAR for intact AAA rose to from 35% in 2001 to 63% in 2005 and comprised 78% of repairs by 2008. During the same period, the number of ruptured AAAs decreased by 40% overall, with nonoperative ruptured AAAs decreasing by 29% and EVAR increasing to 31% of rupture repairs. Hospitals training vascular fellows were quicker to adopt EVAR (2-year lag time) for intact AAA and had higher rates of EVAR for ruptured AAA (41.1% vs 29.2%; P = .001) than did hospitals without fellows. Mortality rates for open repairs of intact (4.0% vs 5.0%; P = .01) and ruptured AAA (34.1% vs 41.0%; P = .031) were lower at fellowship hospitals. The average number of open AAA repairs performed by vascular fellows dropped 50% (44.1 to 21.6/year) from 1999 to 2008.
Conclusions: Contrary to the expectation of a plateau, use of EVAR for intact AAA continues to rise at fellowship and nonfellowship hospitals. Use of EVAR for rupture is being used more often at fellowship programs. The decline in open repairs performed by vascular fellows, and at fellowship and non-fellowship hospitals, may have important implications for future attending experience.
Copyright © 2011. Published by Mosby, Inc.
Figures



References
-
- Parodi JC, Palmaz JC, Barone HD. Transfemoral intraluminal graft implantation for abdominal aortic aneurysms. Ann Vasc Surg. 1991;5:491–499. - PubMed
-
- Schermerhorn ML, O’Malley A, Jhaveri A, Cotterill P, Pomposelli F, Landon BE, et al. Endovascular vs. open repair of abdominal aortic aneurysms in the Medicare population. N Engl J Med. 2008;358:464–474. - PubMed
-
- Schwarze ML, Shen Y, Hemmerich J, Dale W. Age-related trends in utilization and outcome of open and endovascular repair for abdominal aortic aneurysm in the United States, 2001–2006. J Vasc Surg. 2009;50:722–728. e2. - PubMed
-
- Greenhalgh RM, Brown LC, Kwong GP, Powell JT, Thompson SG, et al. Comparison of endovascular aneurysm repair with open repair in patients with abdominal aortic aneurysm (EVAR trial 1), 30-day operative mortality results: randomized controlled trial. Lancet. 2004;364:843–848. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
