

Efficacy of bevacizumab plus erlotinib versus erlotinib alone in advanced non-small-cell lung cancer after failure of standard first-line chemotherapy (BeTa): a double-blind, placebo-controlled, phase 3 trial
- PMID: 21621716
- PMCID: PMC4134127
- DOI: 10.1016/S0140-6736(11)60545-X
Efficacy of bevacizumab plus erlotinib versus erlotinib alone in advanced non-small-cell lung cancer after failure of standard first-line chemotherapy (BeTa): a double-blind, placebo-controlled, phase 3 trial
Abstract
Background: Bevacizumab and erlotinib target different tumour growth pathways with little overlap in their toxic-effect profiles. On the basis of promising results from a phase 1/2 trial assessing safety and activity of erlotinib plus bevacizumab for recurrent or refractory non-small-cell lung cancer (NSCLC), we aimed to assess efficacy and safety of this combination in a phase 3 trial.
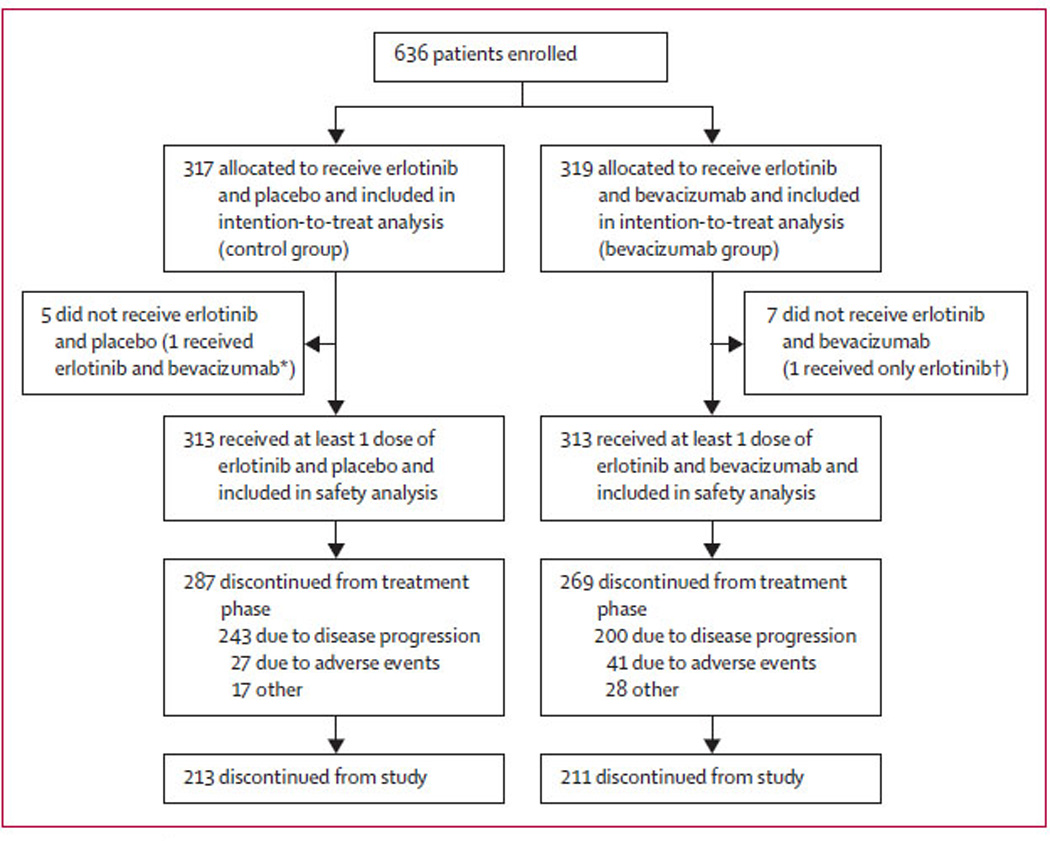
Methods: In our double-blind, placebo-controlled, randomised phase 3 trial (BeTa), we enrolled patients with recurrent or refractory NSCLC who presented to 177 study sites in 12 countries after failure of first-line treatment. Patients were randomly allocated in a one-to-one ratio to receive erlotinib plus bevacizumab (bevacizumab group) or erlotinib plus placebo (control group) according to a computer-generated randomisation sequence by use of an interactive voice response system. The primary endpoint was overall survival in all enrolled patients. Patients, study staff, and investigators were masked to treatment assignment. We assessed safety by calculation of incidence of adverse events and tissue was collected for biomarker analyses. This trial is registered with ClinicalTrials.gov, number NCT00130728.
Findings: Overall survival did not differ between 317 controls and 319 patients in the bevacizumab group (hazard ratio [HR] 0·97, 95% CI 0·80-1·18, p=0·7583). Median overall survival was 9·3 months (IQR 4·1-21·6) for patients in the bevacizumab group compared with 9·2 months (3·8-20·2) for controls. Progression-free survival seemed to be longer in the bevacizumab group (3·4 months [1·4-8·4]) than in the control group (1·7 months [1·3-4·1]; HR 0·62, 95% CI 0·52-0·75) and objective response rate suggested some clinical activity of bevacizumab and erlotinib. However, these secondary endpoint differences could not be defined as significant because the study prespecified that the primary endpoint had to be significant before testing of secondary endpoints could be done, to control type I error rate. In the bevacizumab group, 130 (42%) of 313 patients with safety data had a serious adverse event, compared with 114 (36%) controls. There were 20 (6%) grade 5 adverse events, including two arterial thromboembolic events, in the bevacizumab group, and 14 (4%) in the control group.
Interpretation: Addition of bevacizumab to erlotinib does not improve survival in patients with recurrent or refractory NSCLC.
Funding: Genentech.
Copyright © 2011 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Genentech funded this clinical trial. RSH, LH, PF, and GAO have received funding from Genentech. RSH has consulted for Genentech, OSI, and Roche. GAO has consulted for Genentech and Abraxis. PF has consulted for Genentech, participated in speakers’ bureaux for Genentech and OSI Pharmaceuticals, and grant funding from the Metro Minnesota Community Clinical Oncology Program, a non-profit research program sponsored by NCI. GV has consulted for Genentech and participated in speakers’ bureaux for Genentech and Sanofi-Aventis. C-HS and PO’C have been employed by Genentech and were stockholders with Roche.
Figures



Comment in
-
Salvage with erlotinib plus bevacizumab: not in NSCLC.Lancet. 2011 May 28;377(9780):1810-2. doi: 10.1016/S0140-6736(11)60740-X. Lancet. 2011. PMID: 21621709 No abstract available.
References
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. - PubMed
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010;60:277–300. - PubMed
-
- Pazdur R, Coia LR, Hoskins WJ, Wagman LD. Cancer management: a multidisciplinary approach. 8th edn. Manhasset, NY, USA: CMP Healthcare Media; 2004.
-
- Erlotinib (Tarceva) [package insert] South San Francisco, CA, USA: Genentech;
-
- Shepherd FA, Rodrigues Pereira J, Ciuleanu , et al. Erlotinib in previously treated non-small-cell lung cancer. N Engl J Med. 2005;353:123–132. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
