

Safety of presurgical targeted therapy in the setting of metastatic renal cell carcinoma
- PMID: 21621907
- PMCID: PMC4378825
- DOI: 10.1016/j.eururo.2011.05.032
Safety of presurgical targeted therapy in the setting of metastatic renal cell carcinoma
Abstract
Background: In patients with metastatic renal cell carcinoma (mRCC), the timing of systemic targeted therapy in relation to cytoreductive nephrectomy (CN) is under investigation.
Objective: To evaluate postoperative complications after the use of presurgical targeted therapy prior to CN.
Design, setting, and participants: A retrospective review of all patients who underwent a CN at The University of Texas M.D. Anderson Cancer Center from 2004 to 2010 was performed. Inclusion in this study required documented evidence of mRCC, with treatment incorporating CN.
Interventions: Patients receiving presurgical systemic targeted therapy prior to CN were compared to those undergoing immediate CN.
Measurements: Complications were assessed using the modified Clavien system for a period of 12 mo postoperatively.
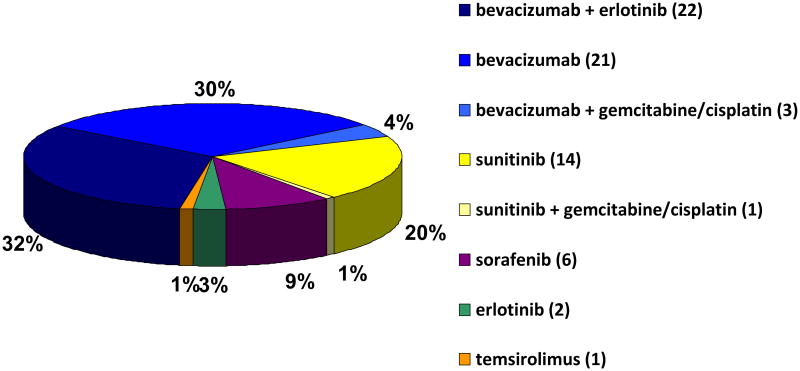
Results and limitations: Presurgical therapy was administered to 70 patients prior to CN (presurgical), while 103 patients had an immediate CN (immediate). A total of 232 complications occurred in 57% of patients (99 of 173). Use of presurgical systemic targeted therapy was predictive of having a complication>90 d postoperatively (p=0.002) and having multiple complications (p=0.013), and it was predictive of having a wound complication (p<0.001). Despite these specific complications, presurgical systemic targeted therapy was not associated with an increased overall complication risk on univariable or multivariate analysis (p=0.064 and p=0.237) and was not predictive for severe (Clavien ≥3) complications (p=0.625). This study is limited by its retrospective nature. As is inherent to any retrospective study reporting on complications, we are limited by reporting bias and the potential for misclassification of specific complications.
Conclusions: Despite an increased risk for specific wound-related complications, overall surgical complications and the risk of severe complications (Clavien ≥3) are not greater after presurgical targeted therapy in comparison to upfront cytoreductive surgery.
Copyright © 2011 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
Safety issues and rationale for neoadjuvant approaches in renal cell carcinoma.Eur Urol. 2011 Nov;60(5):972-4. doi: 10.1016/j.eururo.2011.06.003. Epub 2011 Jun 12. Eur Urol. 2011. PMID: 21684073 No abstract available.
-
Re: Safety of presurgical targeted therapy in the setting of metastatic renal cell carcinoma.J Urol. 2011 Dec;186(6):2209. doi: 10.1016/j.juro.2011.08.104. Epub 2011 Oct 26. J Urol. 2011. PMID: 22078579 No abstract available.
References
-
- Flanigan RC, Salmon SE, Blumenstein BA, et al. Nephrectomy followed by interferon alfa-2b compared with interferon alfa-2b alone for metastatic renal-cell cancer. New Engl J Med. 2001;345:1655–9. - PubMed
-
- Mickisch GH, Garin A, van Poppel H, de Prijck L, Sylvester R. Radical nephrectomy plus interferon-alfa-based immunotherapy compared with interferon alfa alone in metastatic renal-cell carcinoma: a randomised trial. Lancet. 2001;358:966–70. - PubMed
-
- Bex A, Kerst M, Mallo H, Meinhardt W, Horenblas S, de Gast GC. Interferon alpha 2b as medical selection for nephrectomy in patients with synchronous metastatic renal cell carcinoma: a consecutive study. Eur Urol. 2006;49:76–81. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
