

Trends of inpatient spine augmentation: 2001-2008
- PMID: 21622578
- PMCID: PMC7964369
- DOI: 10.3174/ajnr.A2503
Trends of inpatient spine augmentation: 2001-2008
Abstract
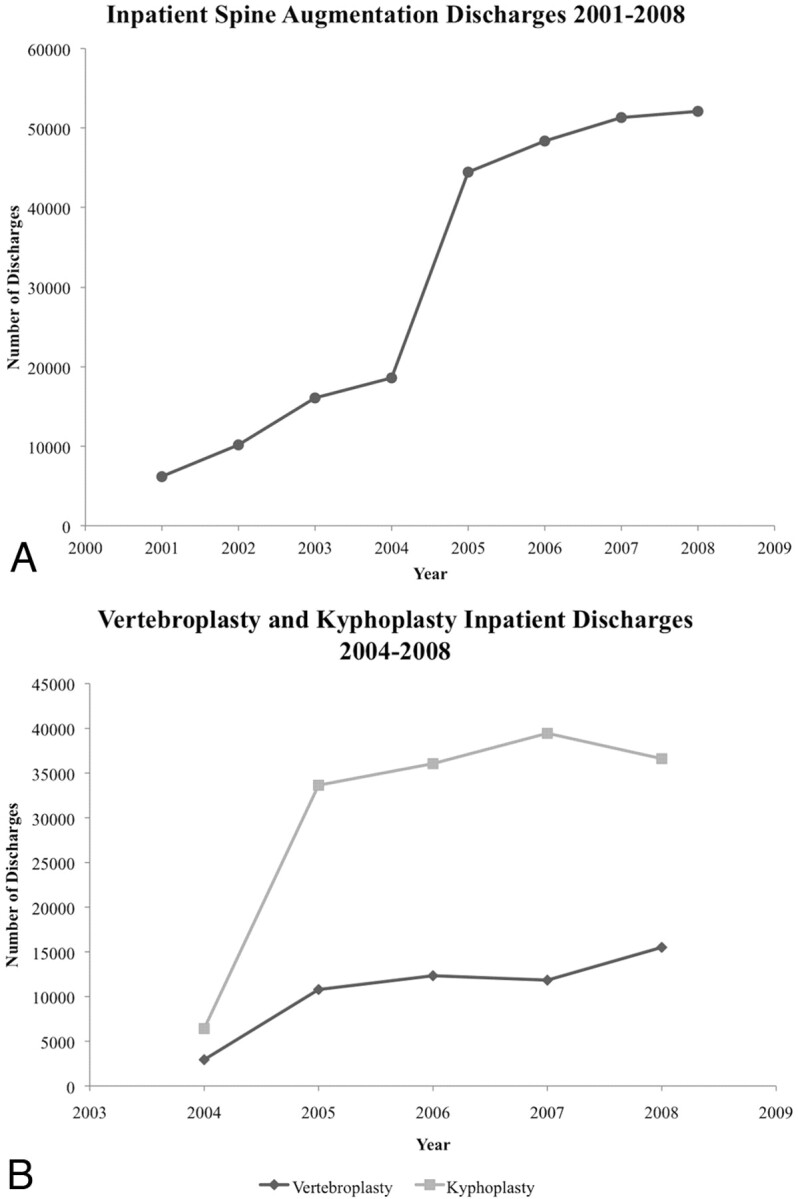
Background and purpose: Vertebroplasty and kyphoplasty are 2 minimally invasive spine augmentation procedures currently used in the management of vertebral compression fractures. Our aim was to examine the NIS data base to identify trends in spine augmentation procedures over time.
Materials and methods: Patients were identified from the NIS data base by using primary diagnosis codes (ICD-9-pathologic vertebral fracture, 733.13) and procedures codes (ICD-9-other repair of bone, 78.49; vertebroplasty, 81.65; kyphoplasty, 81.66). Means and their corresponding standard errors were compared for statistically significant differences by using the Z-test.
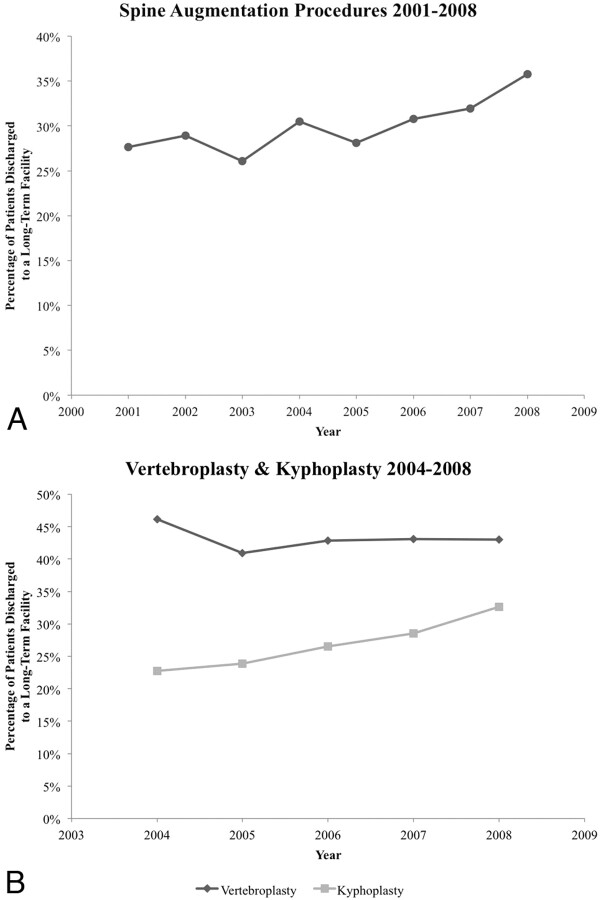
Results: Between 2001 and 2008, >240 000 inpatient spine augmentations were performed in the United States. From 2001 to 2008, there was a 741% increase in the number of hospital discharges for patients who underwent a spine augmentation, but the year-to-year rate of increase has been declining since 2001. From 2004 to 2008, >50 000 inpatient verterbroplasties and >152 000 inpatient kyphoplasties were identified. Compared with vertebroplasty, kyphoplasty patients were less often admitted from the emergency department (33% versus 56%, P < .001), had shorter postaugmentation hospital stays (2.3 versus 3.1 days, P < .001), had fewer comorbidities at presentation (1.4 versus 1.6, P < .01), and were less likely to be discharged to a long-term facility (28% versus 43%, P < .001).
Conclusions: Significant differences were noted in multiple comparisons between vertebroplasty and kyphoplasty, including length of hospital stay and discharges to long-term facilities. However, these findings may simply reflect differences in practice patterns rather than real differences in efficacy between the procedures.
Figures
References
-
- Melton LJ, 3rd, Kallmes DF. Epidemiology of vertebral fractures: implications for vertebral augmentation. Acad Radiol 2006;13:538–45 - PubMed
-
- Garfin SR, Yuan HA, Reiley MA. New technologies in spine: kyphoplasty and vertebroplasty for the treatment of painful osteoporotic compression fractures. Spine (Phila Pa 1976) 2001;26:1511–15 - PubMed
-
- AHRQ. HCUP Nationwide Inpatient Sample (NIS). Healthcare Cost and Utilization Project (HCUP). Rockville, MD; 2001–2008
MeSH terms
LinkOut - more resources
Full Text Sources
Medical