

Goal-directed haemodynamic therapy during elective total hip arthroplasty under regional anaesthesia
- PMID: 21624138
- PMCID: PMC3218998
- DOI: 10.1186/cc10246
Goal-directed haemodynamic therapy during elective total hip arthroplasty under regional anaesthesia
Abstract
Introduction: Total hip replacement is one of the most commonly performed major orthopaedic operations. Goal-directed therapy (GDT) using haemodynamic monitoring has previously demonstrated outcome benefits in high-risk surgical patients under general anaesthesia. GDT has never been formally assessed during regional anaesthesia.
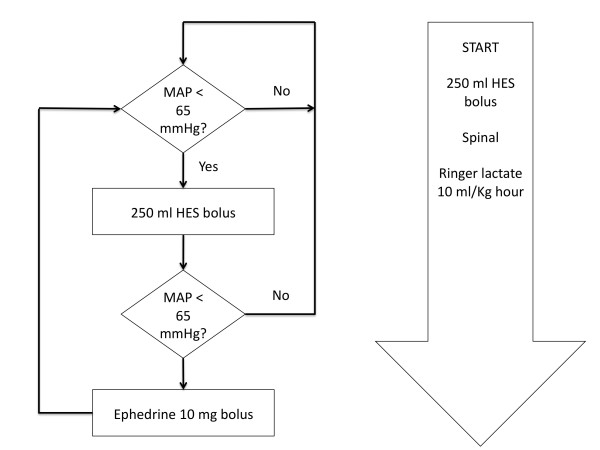
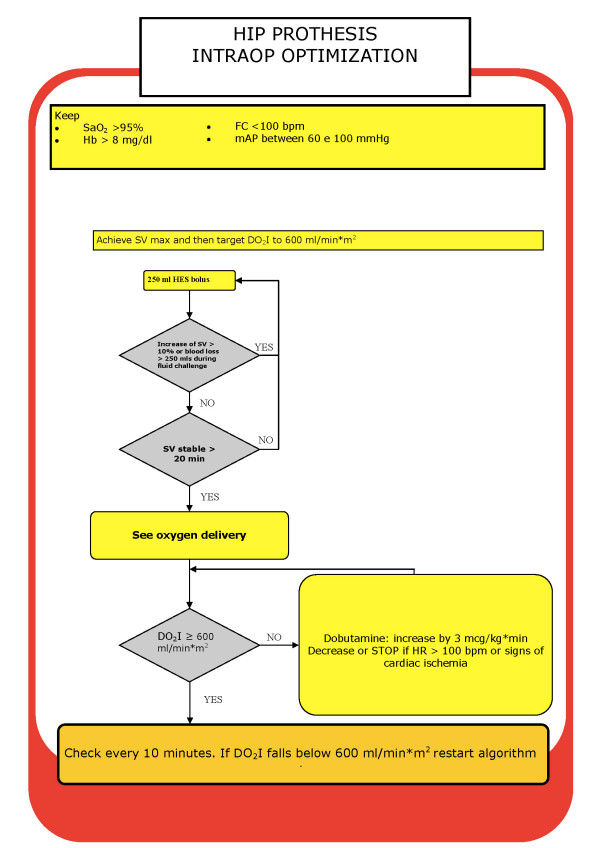
Methods: Patients undergoing total hip replacement while under regional anaesthesia were randomised to either the control group (CTRL) or the protocol group (GDT). Patients in the GDT group, in addition to standard monitoring, were connected to the FloTrac sensor/Vigileo monitor haemodynamic monitoring system, and a GDT protocol was used to maximise the stroke volume and target the oxygen delivery index to > 600 mL/minute/m2.
Results: Patients randomised to the GDT group were given a greater volume of intravenous fluids during the intraoperative period (means ± standard deviation (SD): 6,032 ± 1,388 mL vs. 2,635 ± 346 mL; P < 0.0001), and more of the GDT patients received dobutamine (0 of 20 CTRL patients vs. 11 of 20 GDT patients; P < 0.0003). The GDT patients also received more blood transfused during the intraoperative period (means ± SD: 595 ± 316 mL vs. 0 ± 0 mL; P < 0.0001), although the CTRL group received greater volumes of blood replacement postoperatively (CTRL patients 658 ± 68 mL vs. GDT patients 198 ± 292 mL; P < 0.001). Overall blood consumption (intraoperatively and postoperatively) was not different between the two groups. There were an increased number of complications in the CTRL group (20 of 20 CTRL patients (100%) vs. 16 of 20 GDT patients (80%); P = 0.05). These outcomes were predominantly due to a difference in minor complications (20 of 20 CTRL patients (100%) vs. 15 of 20 GDT patients (75%); P = 0.047).
Conclusions: GDT applied during regional anaesthesia in patients undergoing elective total hip replacement changes intraoperative fluid management and may improve patient outcomes by decreasing postoperative complications. Larger trials are required to confirm our findings.
Figures
Comment in
-
Peri-operative hemodynamic therapy: only large clinical trials can resolve our uncertainty.Crit Care. 2011 Jun 3;15(3):122. doi: 10.1186/cc10011. Crit Care. 2011. PMID: 21639958 Free PMC article.
References
-
- Swanson CE, Day GA, Yelland CE, Broome JR, Massey L, Richardson HR, Dimitri K, Marsh A. The management of elderly patients with femoral fractures: a randomised controlled trial of early intervention versus standard care. Med J Aust. 1998;169:515–518. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
