

Potential utility of conventional MRI signs in diagnosing pseudoprogression in glioblastoma
- PMID: 21624991
- PMCID: PMC3115805
- DOI: 10.1212/WNL.0b013e31821d74e7
Potential utility of conventional MRI signs in diagnosing pseudoprogression in glioblastoma
Abstract
Objective: To examine the potential utility of conventional MRI signs in differentiating pseudoprogression (PsP) from early progression (EP).
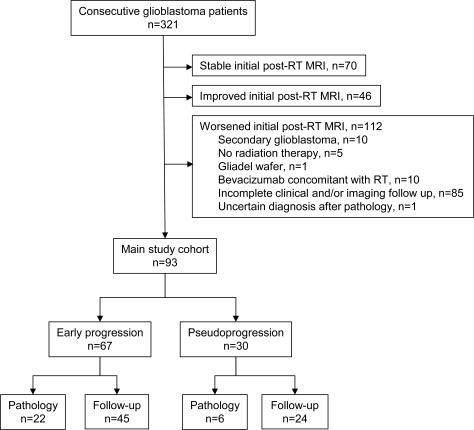
Methods: This retrospective study reviewed initial postradiotherapy MRI scans of 321 patients with glioblastoma undergoing chemotherapy and radiotherapy. A total of 93 patients were found to have new or increased enhancing mass lesions, raising the possibility of PsP. Final diagnosis of PsP or EP was established upon review of surgical specimens from a second resection or by clinical and radiologic follow-up. A total of 11 MRI signs potentially helpful in the differentiation between PsP and EP were examined on the initial post-RT MRI and were correlated with the final diagnosis through χ(2) or Fisher exact test.
Results: Sixty-three (67.7%) of the 93 patients had EP, of which 22 (34.9%) were diagnosed by pathology. Thirty patients (32.3%) had PsP; 6 (16.7% of the 30) were diagnosed by pathology. Subependymal enhancement was predictive for EP (p = 0.001) with 38.1% sensitivity, 93.3% specificity, and 41.8% negative predictive value. The other 10 signs had no predictive value (p = 0.06-1.0).
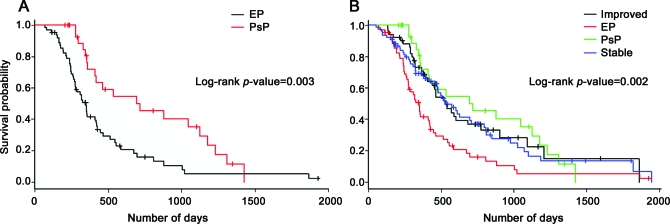
Conclusions: Conventional MRI signs have limited utility in diagnosing PsP in patients with recently treated glioblastomas and worsening enhancing lesions. We did not find a sign with a high negative predictive value for PsP that would have been the most useful for the clinical physician. When present, subependymal spread of the enhancing lesion is a useful MRI marker in identifying EP rather than PsP.
Figures
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 2005;352:987–996 - PubMed
-
- Brandsma D, Stalpers L, Taal W, Sminia P, van den Bent MJ. Clinical features, mechanisms, and management of pseudoprogression in malignant gliomas. Lancet Oncol 2008;9:453–461 - PubMed
-
- Chamberlain MC, Glantz MJ, Chalmers L, Van Horn A, Sloan AE. Early necrosis following concurrent Temodar and radiotherapy in patients with glioblastoma. J Neurooncol 2007;82:81–83 - PubMed
-
- de Wit MC, de Bruin HG, Eijkenboom W, Sillevis Smitt PA, van den Bent MJ. Immediate post-radiotherapy changes in malignant glioma can mimic tumor progression. Neurology 2004;63:535–537 - PubMed
-
- Taal W, Brandsma D, de Bruin HG, et al. Incidence of early pseudo-progression in a cohort of malignant glioma patients treated with chemoirradiation with temozolomide. Cancer 2008;113:405–410 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous