

The use of botulinum toxin A in children with cerebral palsy, with a focus on the lower limb
- PMID: 21629371
- PMCID: PMC2866843
- DOI: 10.1007/s11832-010-0246-x
The use of botulinum toxin A in children with cerebral palsy, with a focus on the lower limb
Abstract
Purpose: The purpose of this review is to clarify the role of botulinum toxin serotype A (BTX-A) in the treatment of children with cerebral palsy (CP), with a special focus on the lower limb.
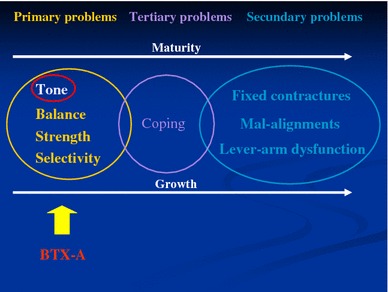
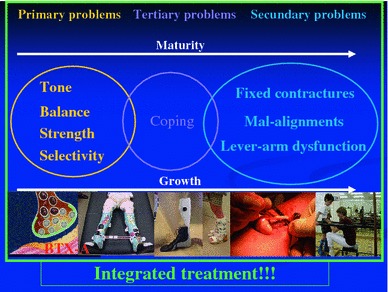
Background: The treatment of spasticity is central in the clinical management of children with CP. BTX-A blocks the release of acetylcholine at the motor end plate, causing a temporary muscular denervation and, in an indirect way, a reduced spasticity. Children with increased tone develop secondary problems over time, such as muscle contractures and bony deformities, which impair their function and which need orthopaedic surgery. However in these younger children, delaying surgery is crucial because the results of early surgical interventions are less predictable and have a higher risk of failure and relapse. As BTX-A treatment reduces tone in a selective way, it allows a better motor control and muscle balance across joints, resulting in an improved range of motion and potential to strengthen antagonist muscles, when started at a young age. The effects are even more obvious when the correct BTX-A application is combined with other conservative therapies, such as physiotherapy, orthotic management and casts. There is now clear evidence that the consequences of persistent increased muscle tone can be limited by applying an integrated multi-level BTX-A treatment approach. Nevertheless, important challenges such as patient selection, defining appropriate individual goals, timing, dosing and dilution, accuracy of injection technique and how to measure outcomes will be questioned. Therefore, "reflection is more important than injection" remains an actual statement.
Keywords: Botulinum toxin A; Cerebral palsy; Lower limb; Multi-level treatment.
Figures
References
-
- Rang M (1993) In: Wenger DR, Rang M (eds) Cerebral palsy in the art and practice of children’s orthopaedics. Raven Press, New York
-
- McManus V, Guillem P, Surman G, Cans C. SCPE work, standardization and definition—an overview of the activities of SCPE: a collaboration of European CP registers. Zhongguo Dang Dai Er Ke Za Zhi. 2006;8(4):261–265. - PubMed
-
- Aoki KR. Immunologic and other properties of therapeutic botulinum toxin serotypes. In: Brin MF, Hallett M, Jankovic J, editors. Scientific and therapeutic aspects of botulinum toxin. Philadelphia: Lippincott Williams & Wilkins; 2002. pp. 103–113.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
