

doi: 10.1055/s-0030-1253517.
Image-guided musculoskeletal biopsies
Affiliations
- PMID: 21629408
- PMCID: PMC3036516
- DOI: 10.1055/s-0030-1253517
Item in Clipboard
Image-guided musculoskeletal biopsies
Semin Intervent Radiol.
2010 Jun.
Abstract
Image-guided musculoskeletal (MSK) biopsies are safe and effective procedures that yield diagnostic accuracies up to 97%. When performed in conjunction with a multidisciplinary team, they provide crucial information that will affect patient care and outcome. Computed tomography and ultrasound are the main modalities used to carry out MSK biopsies, and various needles and techniques are available to help the radiologist perform these procedures safely.
Keywords: Bone; CT; biopsy; ultrasound.
Figures
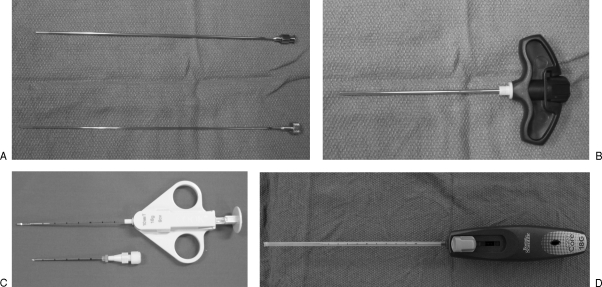
Trephine bone biopsy needles. (A) A 14-gauge bone biopsy needle with inner stylet (Cook, Bloomington, IN). (B) An 11-gauge vertebroplasty needle (Cook) and cutting needles. (C) An 18-gauge QuickCore needle (Cook). (D) An 18-gauge Easycore needle (Boston Scientific, Natick, MA).
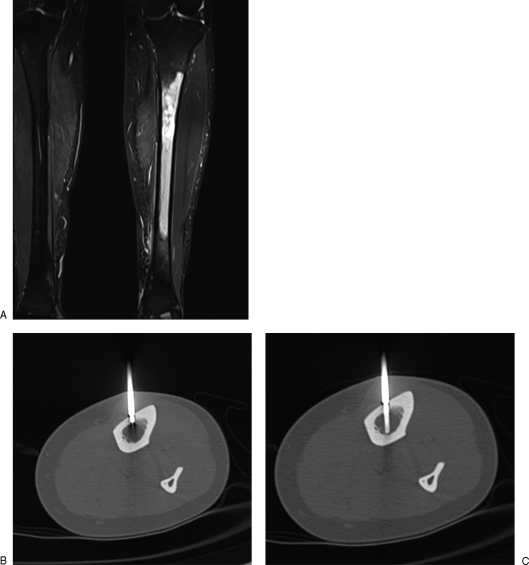
(A) Coronal Short Tau Inversion Recovery (STIR) image shows abnormal left tibial diaphyseal marrow signal targeted for biopsy. (B) Axial computed tomography through tibial diaphysis shows tip of 11-gauge vertebroplasty needle (Cook, Bloomington, IN) used to advance through the cortex and placed adjacent to marrow space, after which the stylet is removed. (C) A 14-gauge bone biopsy needle inserted coaxially into marrow.
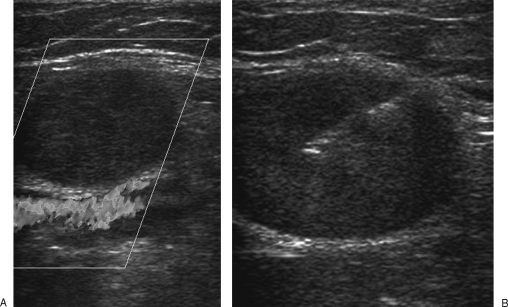
(A) Ultrasound demonstrates a small solid mass abutting the popliteal vessels. (B) A cutting core biopsy needle (the inner stylet is advanced first before the outer cutting sheath is deployed) is used. This reduces the risk of the needle traversing the popliteal vessels and the potential risk of tumor seeding.
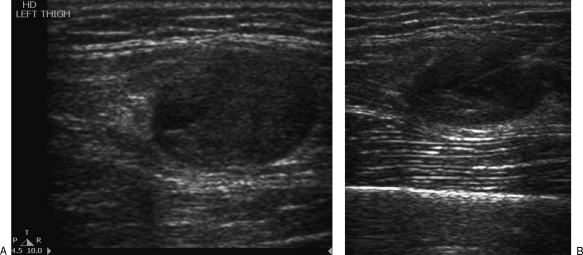
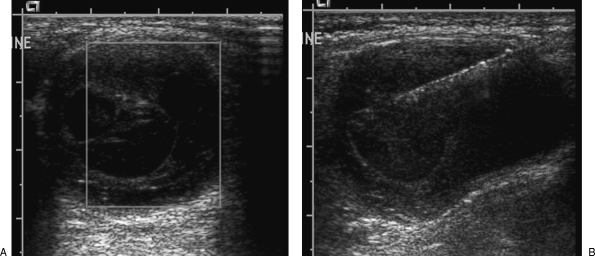
(A) Ultrasound demonstrates a partially cystic soft tissue tumor in the thigh. (B) The core biopsy needle is placed within the solid component of the lesion.
(A) Ultrasound demonstrates a cystic mass in the paraspinal region with several thin internal septations, which demonstrate vascularity on color Doppler. (B) Core biopsy needle targets these septations.
References
-
- Helms C A. “Don't touch” lesions. Philadelphia: WB Saunders; 1995. In: Fundamentals of Skeletal Radiology. 2nd ed. pp. 56–77.
-
- Davies N M, Livesley P J, Cannon S R. Recurrence of an osteosarcoma in a needle biopsy track. J Bone Joint Surg Br. 1993;75:977–978. - PubMed
-
- Schwartz H S, Spengler D M. Needle tract recurrences after closed biopsy for sarcoma: three cases and review of the literature. Ann Surg Oncol. 1997;4:228–236. - PubMed
-
- Wafa H, Grimer R J. Surgical options and outcomes in bone sarcoma. Expert Rev Anticancer Ther. 2006;6:239–248. - PubMed
