

Rectocele
- PMID: 21629626
- PMCID: PMC2967328
- DOI: 10.1055/s-0030-1254295
Rectocele
Abstract
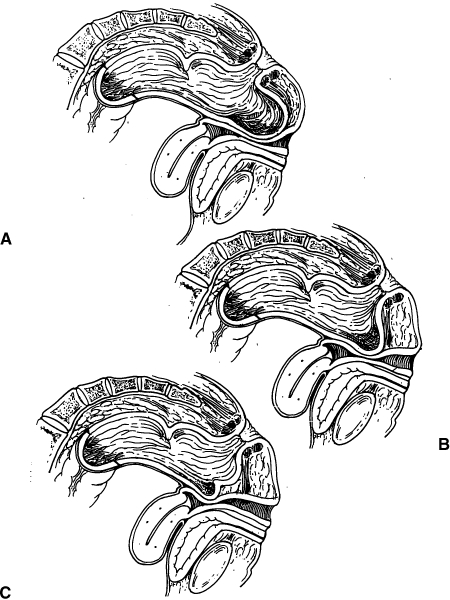
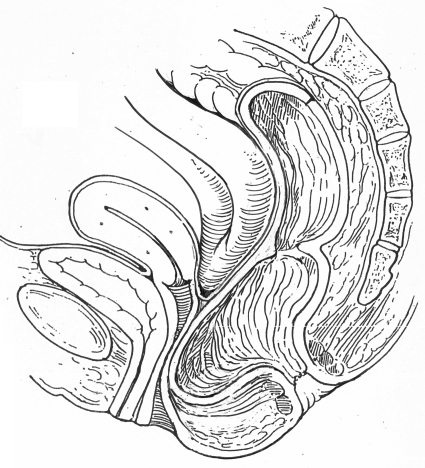
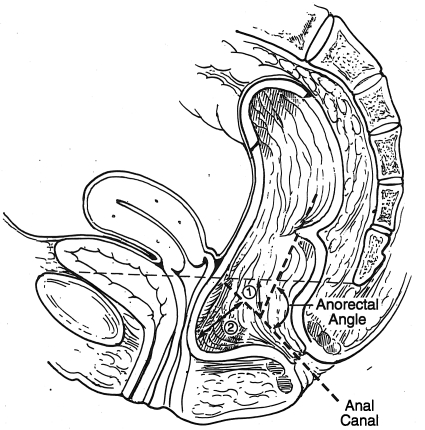
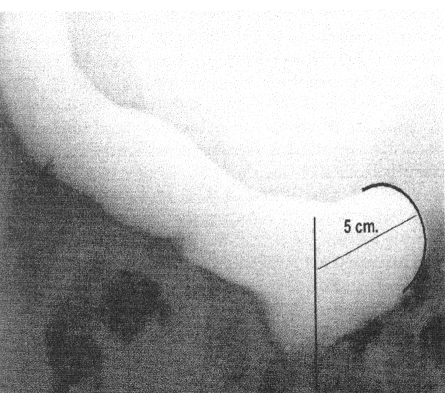
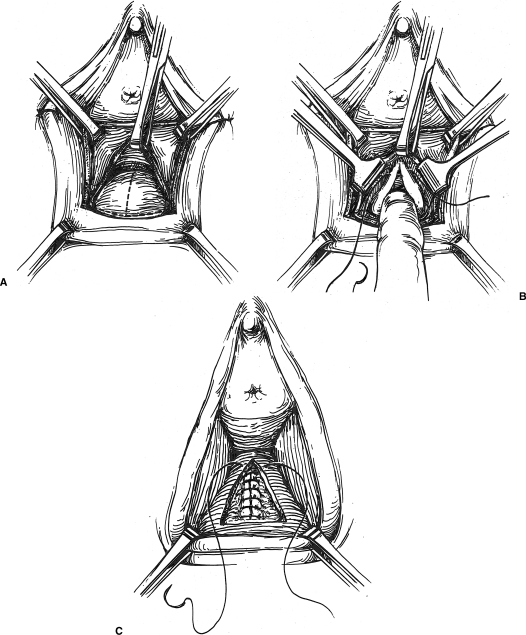
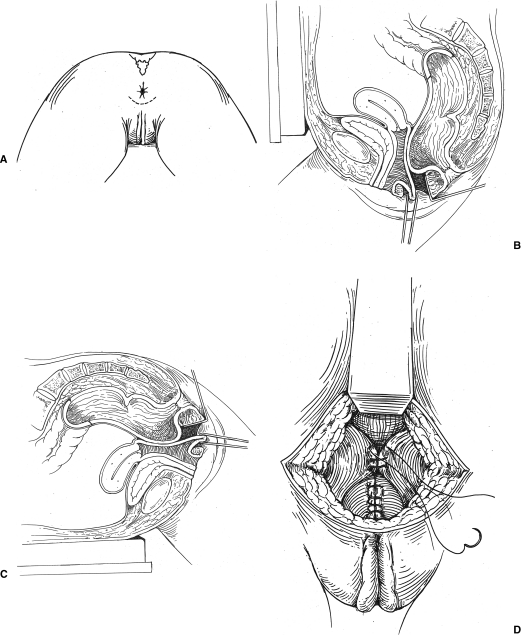
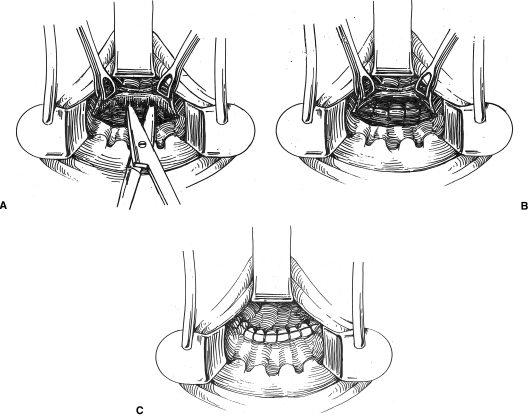
Rectoceles are common and involve a herniation of the rectum into the posterior vaginal wall that results in a vaginal bulge. Women with rectoceles generally complain of perineal and vaginal pressure, obstructive defecation, constipation, or the need to splint or digitally reduce the vagina to effectuate a bowel movement. Rectoceles are associated with age and parturition and arise from either a tear or stretching of the rectovaginal fascia, and can be repaired via a vaginal, anal, or perineal approach. Although the rate of successful anatomic repair is high, reports of functional outcome are more variable.
Keywords: Rectocele; defecation disorders; posterior colporrhaphy.
Figures
References
-
- Rosato G O. In Beck DE, Wexner SD, editor. Fundamentals of Anorectal Surgery. London: WB Saunders; 1998. Rectocele and perineal hernias. pp. 187–197.
-
- Pollak J, Davila G W. Rectocele repair: the gynecologic approach. Clin Colon Rectal Surg. 2003;16:61–69.
-
- Richardson A C. The rectovaginal septum revisited: its relationship to rectocele and its importance in rectocele repair. Clin Obstet Gynecol. 1993;36(4):976–983. - PubMed
-
- Uhlenhuth E, Wolfe W M, Smith E M, Middleton E B. The rectogenital septum. Surg Gynecol Obstet. 1948;86(2):148–163. - PubMed
-
- Milley P S, Nichols D H. A correlative investigation of the human rectovaginal septum. Anat Rec. 1969;163(3):443–451. - PubMed
