

The use of a mobile laboratory unit in support of patient management and epidemiological surveillance during the 2005 Marburg Outbreak in Angola
- PMID: 21629730
- PMCID: PMC3101190
- DOI: 10.1371/journal.pntd.0001183
The use of a mobile laboratory unit in support of patient management and epidemiological surveillance during the 2005 Marburg Outbreak in Angola
Abstract
Background: Marburg virus (MARV), a zoonotic pathogen causing severe hemorrhagic fever in man, has emerged in Angola resulting in the largest outbreak of Marburg hemorrhagic fever (MHF) with the highest case fatality rate to date.
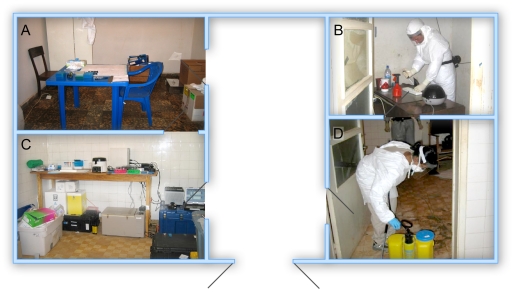
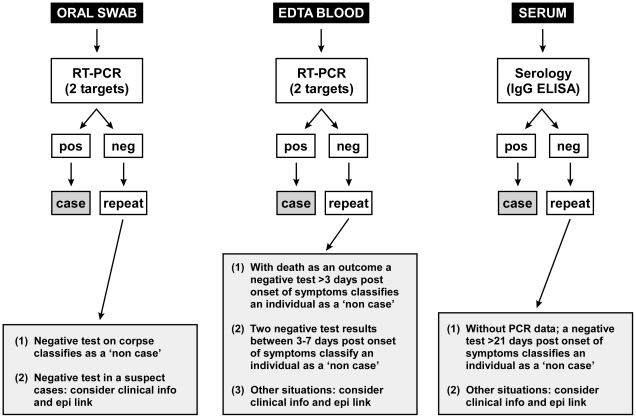
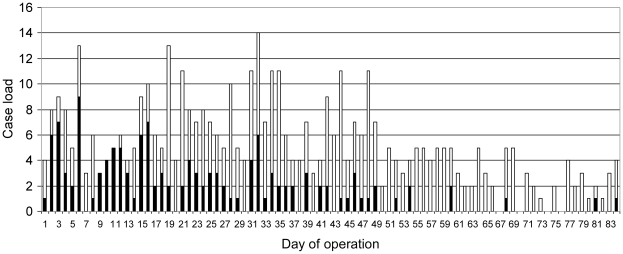
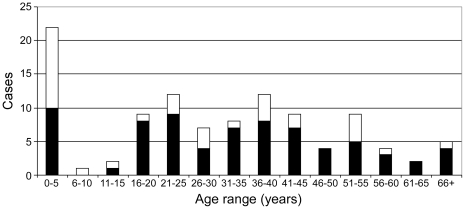
Methodology/principal findings: A mobile laboratory unit (MLU) was deployed as part of the World Health Organization outbreak response. Utilizing quantitative real-time PCR assays, this laboratory provided specific MARV diagnostics in Uige, the epicentre of the outbreak. The MLU operated over a period of 88 days and tested 620 specimens from 388 individuals. Specimens included mainly oral swabs and EDTA blood. Following establishing on site, the MLU operation allowed a diagnostic response in <4 hours from sample receiving. Most cases were found among females in the child-bearing age and in children less than five years of age. The outbreak had a high number of paediatric cases and breastfeeding may have been a factor in MARV transmission as indicated by the epidemiology and MARV positive breast milk specimens. Oral swabs were a useful alternative specimen source to whole blood/serum allowing testing of patients in circumstances of resistance to invasive procedures but limited diagnostic testing to molecular approaches. There was a high concordance in test results between the MLU and the reference laboratory in Luanda operated by the US Centers for Disease Control and Prevention.
Conclusions/significance: The MLU was an important outbreak response asset providing support in patient management and epidemiological surveillance. Field laboratory capacity should be expanded and made an essential part of any future outbreak investigation.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Feldmann H, Geisbert TW, Jahrling PB, Klenk HD, Netesov SV, et al. Filoviridae. In: Fauquet CM, Mayo MA, Maniloff J, Desselberger U, Ball LA, editors. Virus Taxonomy: VIIIth Report of the International Committee on Taxonomy of Viruses. London, UK: Elsevire/Academic Press; 2005. pp. 645–653.
-
- Sanchez A, Geisbert TW, Feldmann H. Filoviridae: Marburg and Ebola viruses. In: Knipe DM, Howley PM, Griffin DE, Lamb A, Martin MA, Roizman B, Strauss SE, editors. Fields Virology. Philadelphia: Lippincott, Williams and Wilkins; 2007. pp. 1409–1448. 5th ed.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
