

Lenalidomide, cyclophosphamide and dexamethasone (CRd) for newly diagnosed multiple myeloma: results from a phase 2 trial
- PMID: 21630308
- PMCID: PMC3901994
- DOI: 10.1002/ajh.22053
Lenalidomide, cyclophosphamide and dexamethasone (CRd) for newly diagnosed multiple myeloma: results from a phase 2 trial
Abstract
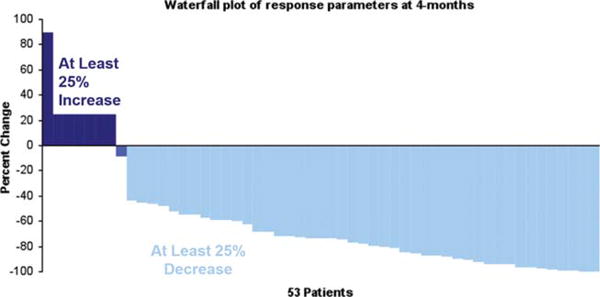
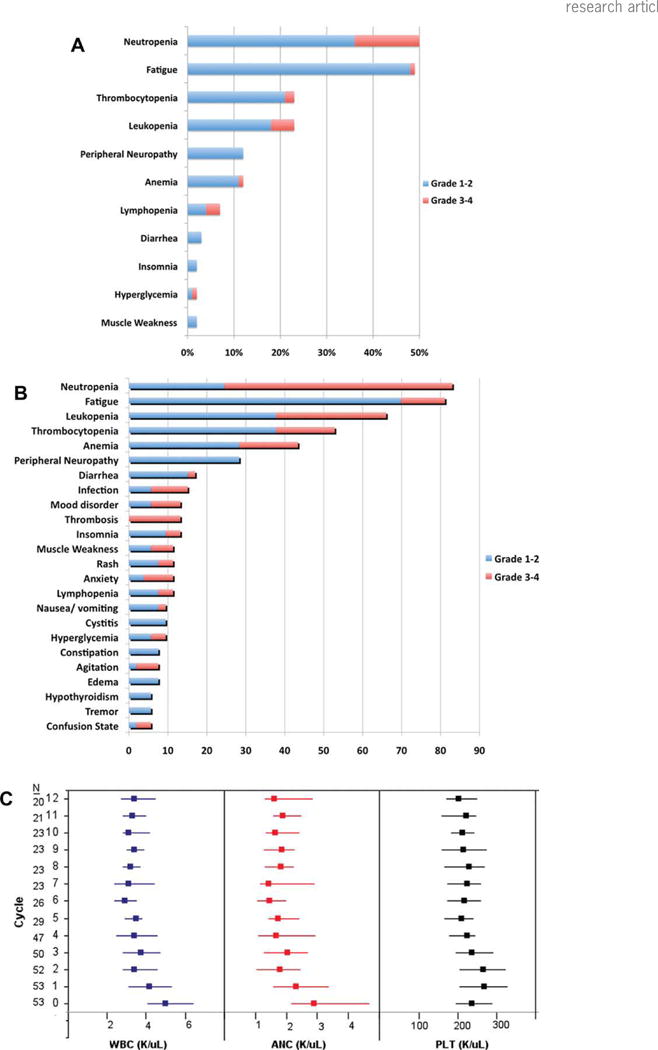
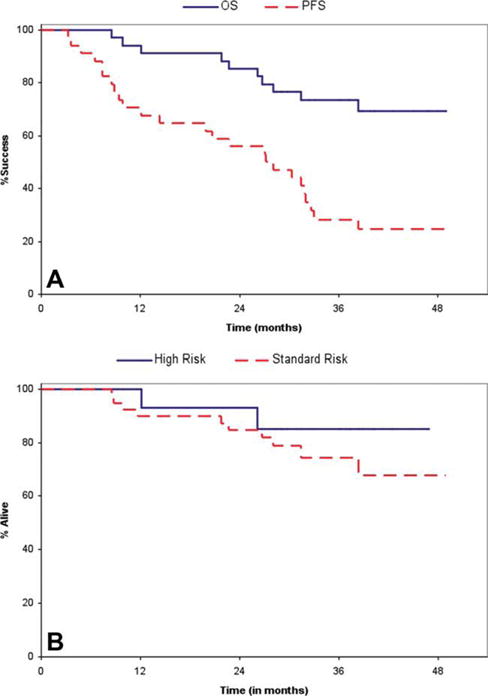
The combination of lenalidomide and low-dose dexamethasone is an effective treatment for multiple myeloma (MM). Addition of alkylating agents to lenalidomide or thalidomide results in increased response rates and deeper responses. We designed this trial to study the combination of cyclophosphamide, lenalidomide, and dexamethasone (CRd) as initial therapy for MM. Fifty-three patients with previously untreated symptomatic MM was enrolled. Patients received 4-week treatment cycles consisting of lenalidomide (25 mg daily for 3 weeks), dexamethasone (40 mg weekly), and cyclophosphamide (300 mg/m(2) weekly for 3 weeks). A partial response or better was seen in 85% of patients including 47% with a very good partial response or better. The toxicities were manageable with over 80% of planned doses delivered; six patients went off study for toxicity. The median progression free survival (PFS) for the entire group was 28 months (95% CI: 22.7-32.6) and the overall survival (OS) at 2 years was 87% (95% CI: 78-96). Importantly, 14 patients with high-risk MM had similar PFS and OS as the standard-risk patients (n = 39). CRd is an effective and well-tolerated regimen for upfront therapy of MM with high response rates and excellent 2-year OS, and is suitable for long-term therapy.
Trial registration: ClinicalTrials.gov NCT00478218.
Copyright © 2011 Wiley-Liss, Inc.
Conflict of interest statement
Figures
References
-
- Kumar S. Multiple myeloma-current issues and controversies. Cancer Treat Rev. 2010;36(Suppl 2):S3–11. - PubMed
-
- Richardson PG, Barlogie B, Berenson J, et al. A phase 2 study of bortezomib in relapsed, refractory myeloma. N Engl J Med. 2003;348:2609–2617. - PubMed
-
- Rajkumar SV, Blood E, Vesole D, et al. Phase III clinical trial of thalidomide plus dexamethasone compared with dexamethasone alone in newly diagnosed multiple myeloma: A clinical trial coordinated by the Eastern Cooperative Oncology Group. J Clin Oncol. 2006;24:431–436. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical