

Surgical management of tumors producing the thalamopeduncular syndrome of childhood
- PMID: 21631193
- PMCID: PMC3531960
- DOI: 10.3171/2011.4.PEDS119
Surgical management of tumors producing the thalamopeduncular syndrome of childhood
Abstract
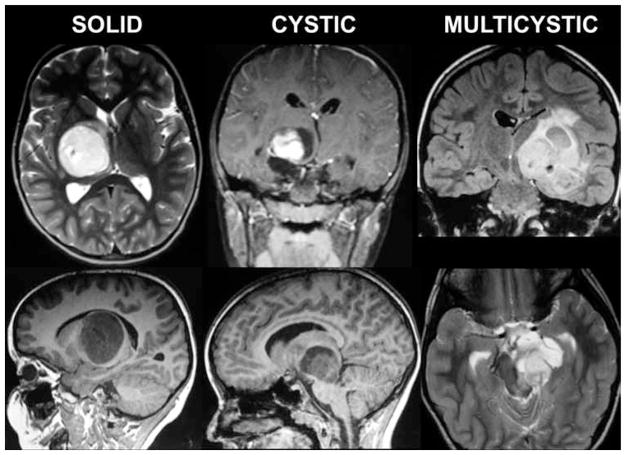
Object: Thalamopeduncular tumors arise at the junction of the inferior thalamus and cerebral peduncle and present with a common clinical syndrome of progressive spastic hemiparesis. Pathologically, these lesions are usually juvenile pilocytic astrocytomas and are best treated with resection with the intent to cure. The goals of this study are to define a common clinical syndrome produced by thalamopeduncular tumors and to discuss imaging characteristics as well as surgical adjuncts, intraoperative nuances, and postoperative complications relating to the resection of these neoplasms.
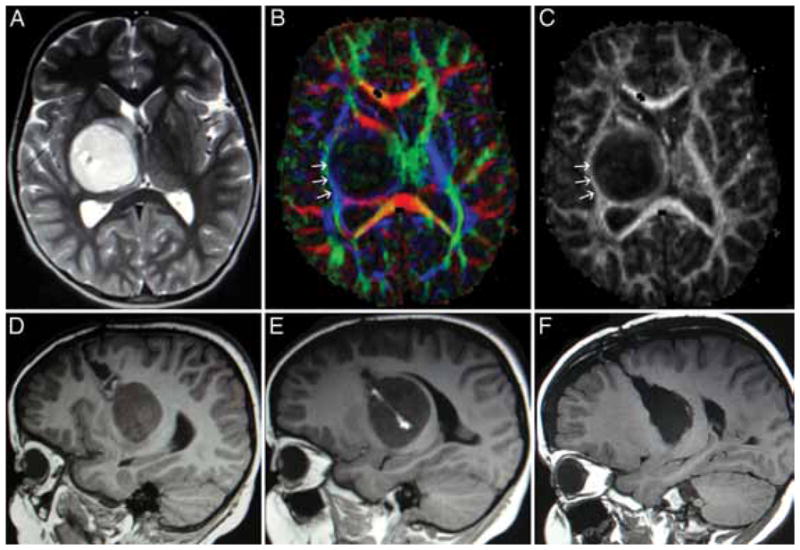
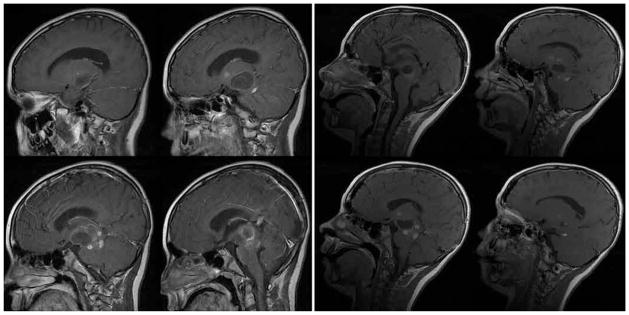
Methods: The authors present a retrospective review of their experience with 10 children presenting between 3 and 15 years of age with a thalamopeduncular syndrome. Formal preoperative MR imaging was obtained in all patients, and diffusion tensor (DT) imaging was performed in 9 patients. Postoperative MR imaging was obtained to evaluate the extent of tumor resection. A prospective analysis of clinical outcomes was then conducted by the senior author.
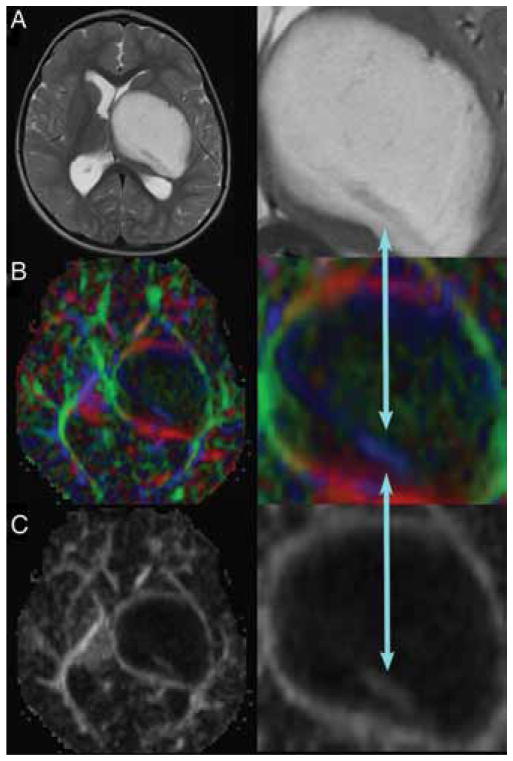
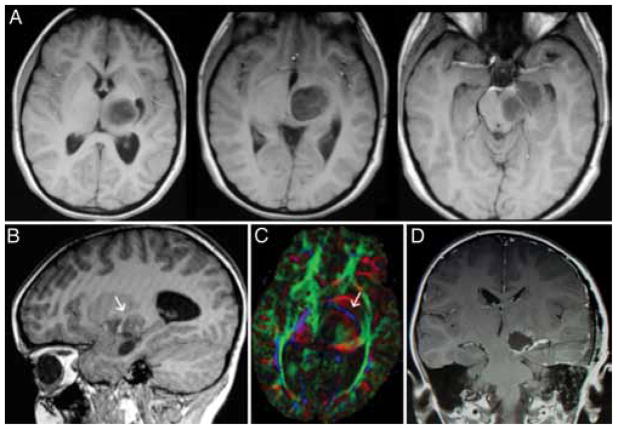
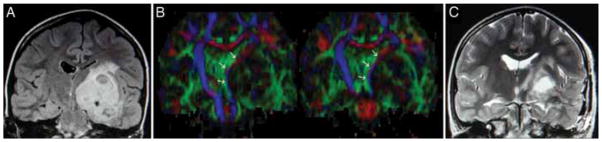
Results: Pilocytic astrocytoma was the pathological diagnosis in 9 cases, and the other was fibrillary astrocytoma. Seven of 9 pilocytic astrocytomas were completely resected. Radical surgery was avoided in 1 child after DT imaging revealed that the corticospinal tract (CST) coursed through the center of the tumor, consistent with the infiltrative nature of fibrillary astrocytoma as identified by stereotactic biopsy. In 8 patients, tractography served as an important adjunct for designing a surgical approach that spared the CST. In 6 cases the CSTs were pushed anterolaterally, making a transsylvian approach a poor choice, as was evidenced by the first patient in the series, who underwent operation prior to the advent of tractography, and who awoke with a dense contralateral hemiparesis. Thus, subsequent patients with this deviation pattern underwent a transcortical approach via the middle temporal gyrus. One patient exhibited medial deviation of the tracts and another had lateral deviation, facilitating a transtemporal and a transfrontal approach, respectively.
Conclusions: The thalamopeduncular syndrome of progressive spastic hemiparesis presenting in children with or without symptoms of headache should alert the examiner to the possibility of a tumoral involvement of CSTs. Preoperative tractography is a useful adjunct to surgical planning in tumors that displace motor pathways. Gross-total resection of pilocytic astrocytomas usually results in cure, and therefore should be entertained when developing a treatment strategy for thalamopeduncular tumors of childhood.
Conflict of interest statement
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Figures
References
-
- Barkovich AJ. Pediatric Neuroimaging. 3. Philadelphia: Lippincott Williams & Wilkins; 2000.
-
- Berman JI, Berger MS, Chung SW, Nagarajan SS, Henry RG. Accuracy of diffusion tensor magnetic resonance imaging tractography assessed using intraoperative subcortical stimulation mapping and magnetic source imaging. J Neurosurg. 2007;107:488–494. - PubMed
-
- Bernstein M, Hoffman HJ, Halliday WC, Hendrick EB, Humphreys RP. Thalamic tumors in children. Long-term followup and treatment guidelines. J Neurosurg. 1984;61:649–656. - PubMed
-
- Cuccia V, Monges J. Thalamic tumors in children. Childs Nerv Syst. 1997;13:514–521. - PubMed
-
- DaSilva AF, Tuch DS, Wiegell MR, Hadjikhani N. A primer on diffusion tensor imaging of anatomical substructures. Neurosurg Focus. 2003;15(1):E4. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
