

Detection of blast-related traumatic brain injury in U.S. military personnel
- PMID: 21631321
- PMCID: PMC3146351
- DOI: 10.1056/NEJMoa1008069
Detection of blast-related traumatic brain injury in U.S. military personnel
Abstract
Background: Blast-related traumatic brain injuries have been common in the Iraq and Afghanistan wars, but fundamental questions about the nature of these injuries remain unanswered.
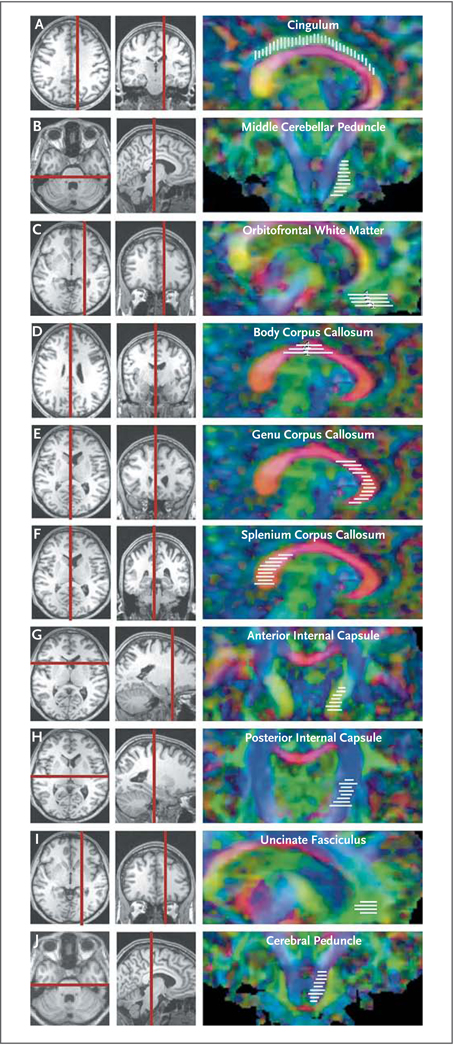
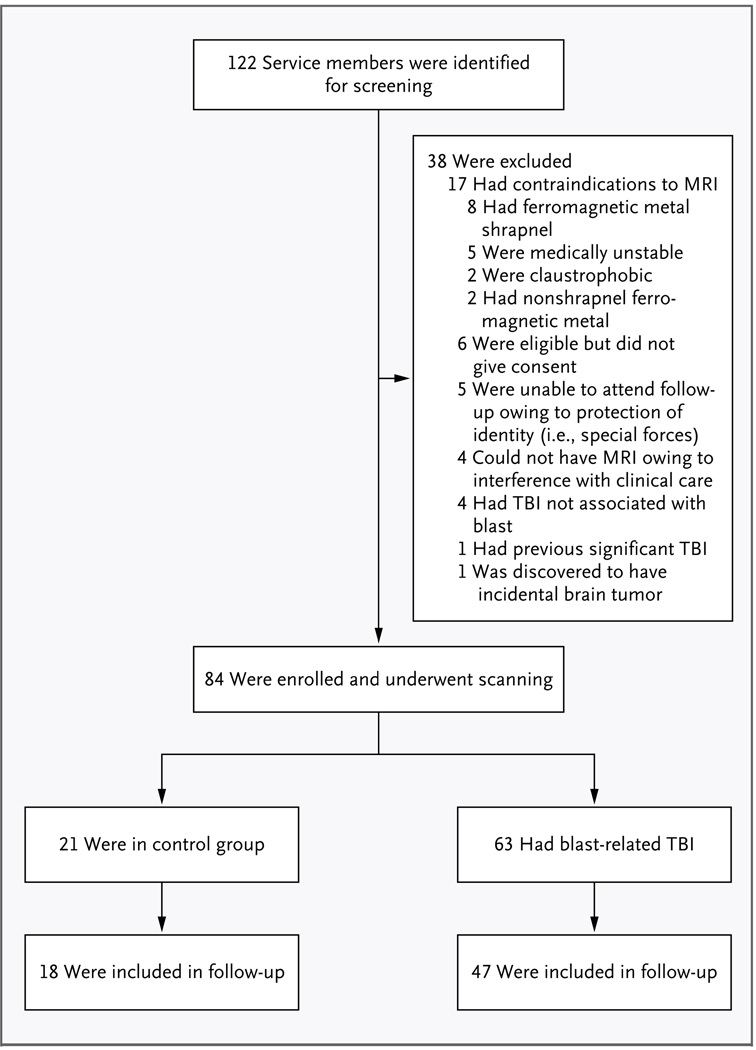
Methods: We tested the hypothesis that blast-related traumatic brain injury causes traumatic axonal injury, using diffusion tensor imaging (DTI), an advanced form of magnetic resonance imaging that is sensitive to axonal injury. The subjects were 63 U.S. military personnel who had a clinical diagnosis of mild, uncomplicated traumatic brain injury. They were evacuated from the field to the Landstuhl Regional Medical Center in Landstuhl, Germany, where they underwent DTI scanning within 90 days after the injury. All the subjects had primary blast exposure plus another, blast-related mechanism of injury (e.g., being struck by a blunt object or injured in a fall or motor vehicle crash). Controls consisted of 21 military personnel who had blast exposure and other injuries but no clinical diagnosis of traumatic brain injury.
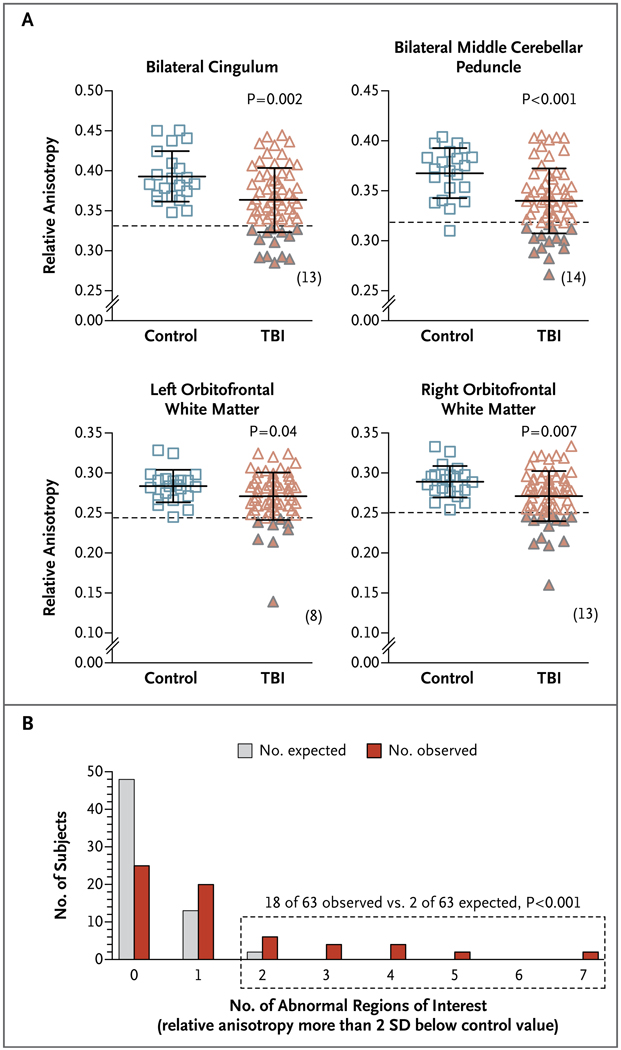
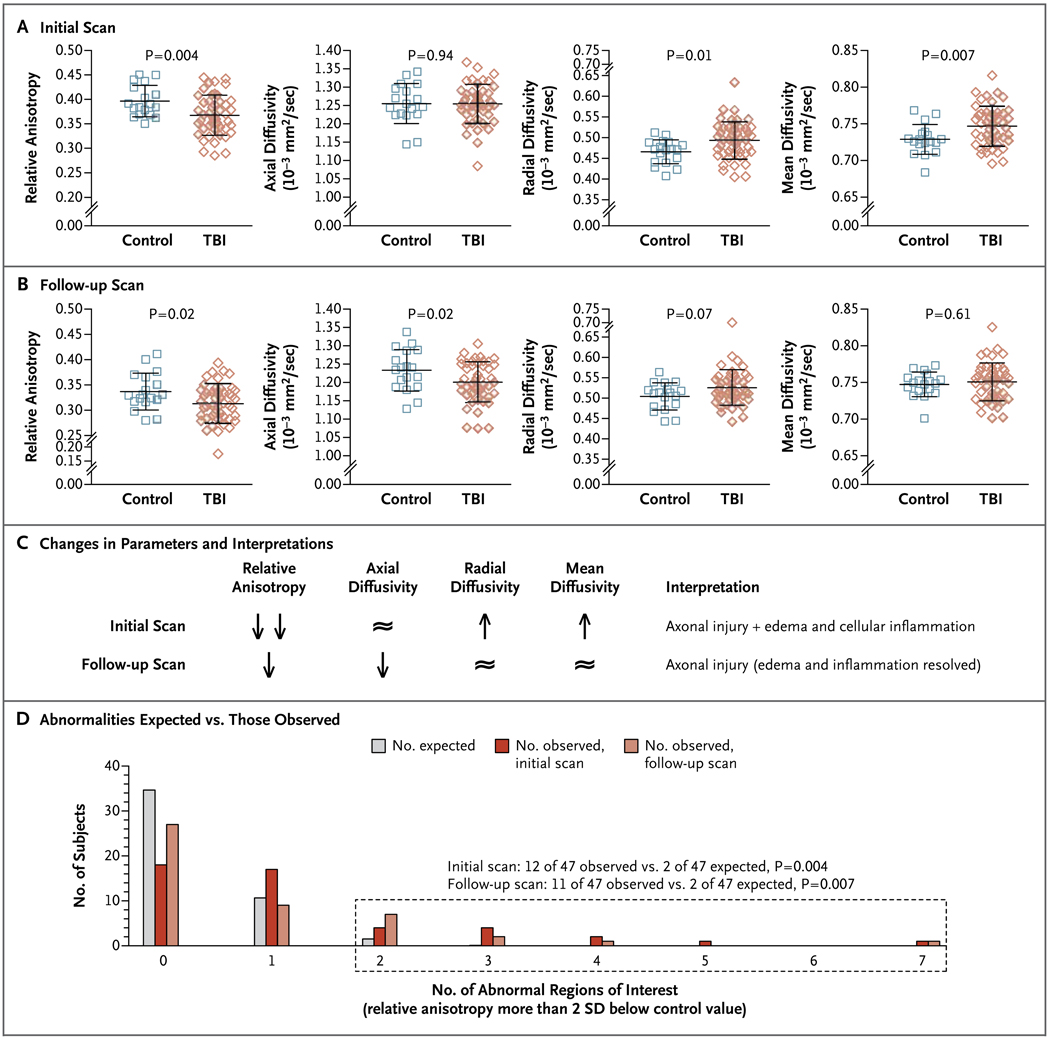
Results: Abnormalities revealed on DTI were consistent with traumatic axonal injury in many of the subjects with traumatic brain injury. None had detectable intracranial injury on computed tomography. As compared with DTI scans in controls, the scans in the subjects with traumatic brain injury showed marked abnormalities in the middle cerebellar peduncles (P<0.001), in cingulum bundles (P=0.002), and in the right orbitofrontal white matter (P=0.007). In 18 of the 63 subjects with traumatic brain injury, a significantly greater number of abnormalities were found on DTI than would be expected by chance (P<0.001). Follow-up DTI scans in 47 subjects with traumatic brain injury 6 to 12 months after enrollment showed persistent abnormalities that were consistent with evolving injuries.
Conclusions: DTI findings in U.S. military personnel support the hypothesis that blast-related mild traumatic brain injury can involve axonal injury. However, the contribution of primary blast exposure as compared with that of other types of injury could not be determined directly, since none of the subjects with traumatic brain injury had isolated primary blast injury. Furthermore, many of these subjects did not have abnormalities on DTI. Thus, traumatic brain injury remains a clinical diagnosis. (Funded by the Congressionally Directed Medical Research Program and the National Institutes of Health; ClinicalTrials.gov number, NCT00785304.).
Figures
Comment in
-
Brain injuries from blasts.N Engl J Med. 2011 Jun 2;364(22):2156-7. doi: 10.1056/NEJMe1102187. N Engl J Med. 2011. PMID: 21631329 No abstract available.
-
Blast-related traumatic brain injury in U.S. military personnel.N Engl J Med. 2011 Sep 1;365(9):860; author reply 860-1. doi: 10.1056/NEJMc1107891. N Engl J Med. 2011. PMID: 21879907 No abstract available.
-
Blast-related traumatic brain injury in U.S. military personnel.N Engl J Med. 2011 Sep 1;365(9):860. doi: 10.1056/NEJMc1107891. N Engl J Med. 2011. PMID: 21879908 No abstract available.
-
Blast-related traumatic brain injury in U.S. military personnel.N Engl J Med. 2011 Sep 1;365(9):859; author reply 860-1. doi: 10.1056/NEJMc1107891. N Engl J Med. 2011. PMID: 21879909 No abstract available.
References
-
- Tanielian TL, Jaycox LH, editors. Invisible wounds of war: psychological and cognitive injuries, their consequences, and services to assist recovery. Santa Monica, CA: RAND; 2008.
-
- Casscells SW. Traumatic brain injury: definition and reporting. Washington, DC: Department of Defense; 2007. Oct, (memorandum). ( http://mhs.osd.mil/Content/docs/pdfs/policies/2007/07-030.pdf.)
-
- Hoge CW, McGurk D, Thomas JL, Cox AL, Engel CC, Castro CA. Mild traumatic brain injury in U.S. soldiers returning from Iraq. N Engl J Med. 2008;358:453–463. - PubMed
-
- Jones E, Fear NT, Wessely S. Shell shock and mild traumatic brain injury: a historical review. Am J Psychiatry. 2007;164:1641–1645. - PubMed
-
- Blumbergs PC, Scott G, Manavis J, Wainwright H, Simpson DA, McLean AJ. Staining of amyloid precursor protein to study axonal damage in mild head injury. Lancet. 1994;344:1055–1056. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials