

Trends in hospital volume and operative mortality for high-risk surgery
- PMID: 21631325
- PMCID: PMC3150488
- DOI: 10.1056/NEJMsa1010705
Trends in hospital volume and operative mortality for high-risk surgery
Abstract
Background: There were numerous efforts in the United States during the previous decade to concentrate selected surgical procedures in high-volume hospitals. It remains unknown whether referral patterns for high-risk surgery have changed as a result and how operative mortality has been affected.
Methods: We used national Medicare data to study patients undergoing one of eight different cancer and cardiovascular operations from 1999 through 2008. For each procedure, we examined trends in hospital volume and market concentration, defined as the proportion of Medicare patients undergoing surgery in the top decile of hospitals by volume per year. We used regression-based techniques to assess the effects of volume and market concentration on mortality over time, adjusting for case mix.
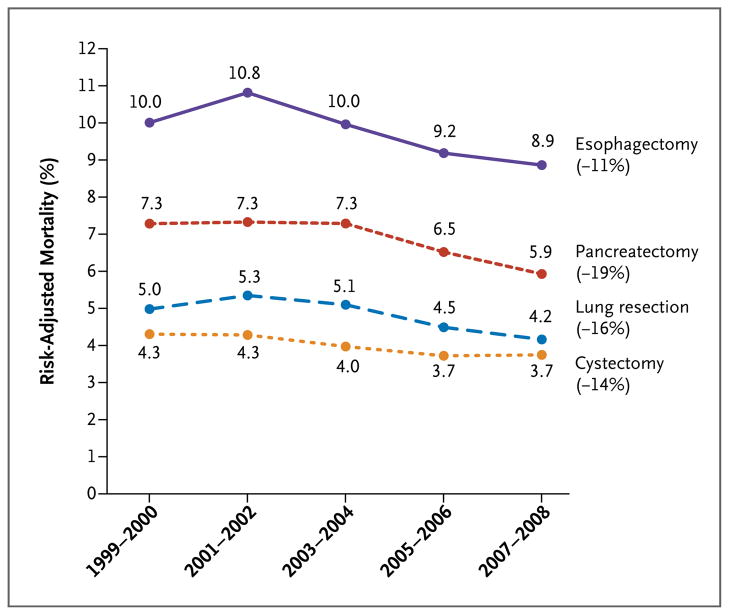
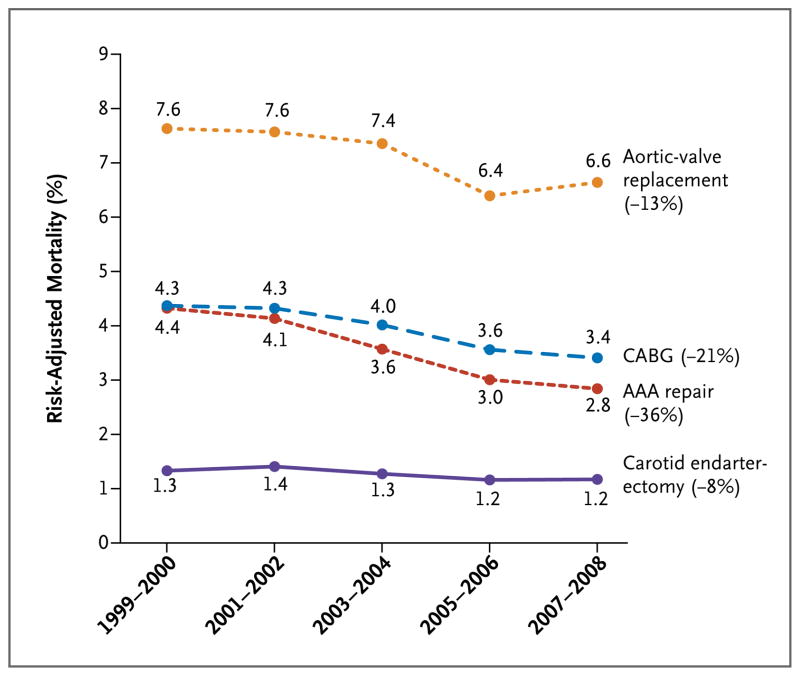
Results: Median hospital volumes of four cancer resections (lung, esophagus, pancreas, and bladder) and of repair of abdominal aortic aneurysm (AAA) rose substantially. Depending on the procedure, higher hospital volumes were attributable to an increasing number of cases nationwide, an increasing market concentration, or both. Hospital volumes rose slightly for aortic-valve replacement but fell for coronary-artery bypass grafting and carotid endarterectomy. Operative mortality declined for all eight procedures, ranging from a relative decline of 8% for carotid endarterectomy (1.3% mortality in 1999 and 1.2% in 2008) to 36% for AAA repair (4.4% in 1999 and 2.8% in 2008). Higher hospital volumes explained a large portion of the decline in mortality for pancreatectomy (67% of the decline), cystectomy (37%), and esophagectomy (32%), but not for the other procedures.
Conclusions: Operative mortality with high-risk surgery fell substantially during the previous decade. Although increased market concentration and hospital volume have contributed to declining mortality with some high-risk cancer operations, declines in mortality with other procedures are largely attributable to other factors. (Funded by the National Institute on Aging.).
Figures
Comment in
-
[High volume and operative mortality].Chirurg. 2012 Jan;83(1):77-8. doi: 10.1007/s00104-011-2185-6. Chirurg. 2012. PMID: 22033895 German. No abstract available.
-
Words of Wisdom: re: trends in hospital volume and operative mortality for high-risk surgery.Eur Urol. 2013 Mar;63(3):582. doi: 10.1016/j.eururo.2012.12.010. Eur Urol. 2013. PMID: 23357894 No abstract available.
References
-
- Committee on Quality of Health Care in America and the National Cancer Policy Board. Interpreting the volume–outcome relationship in the context of health care quality. Washington, DC: Institute of Medicine; 2000.
-
- Birkmeyer JD, Siewers AE, Finlayson EV, et al. Hospital volume and surgical mortality in the United States. N Engl J Med. 2002;346:1128–37. - PubMed
-
- Dudley RA, Johansen KL, Brand R, Rennie DJ, Milstein A. Selective referral to high-volume hospitals: estimating potentially avoidable deaths. JAMA. 2000;283:1159–66. - PubMed
-
- Milstein A, Galvin RS, Delbanco SF, Salber P, Buck CR., Jr Improving the safety of health care: the Leapfrog Initiative. Eff Clin Pract. 2000;3:313–6. [Erratum, Eff Clin Pract 2001;4:94.] - PubMed
-
- American College of Surgeons Bariatric Surgery Center Network. home page( http://www.acsbscn.org/Public/index.jsp.) - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical