

Influence of immunosuppressive treatment on risk of recurrent malignancy after allogeneic hematopoietic cell transplantation
- PMID: 21633087
- PMCID: PMC3138695
- DOI: 10.1182/blood-2011-01-330217
Influence of immunosuppressive treatment on risk of recurrent malignancy after allogeneic hematopoietic cell transplantation
Abstract
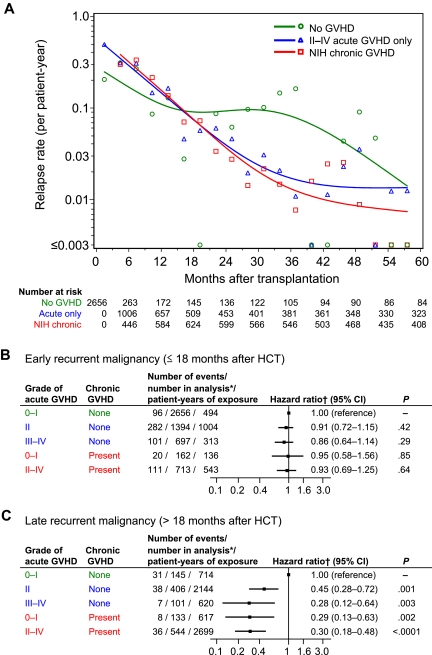
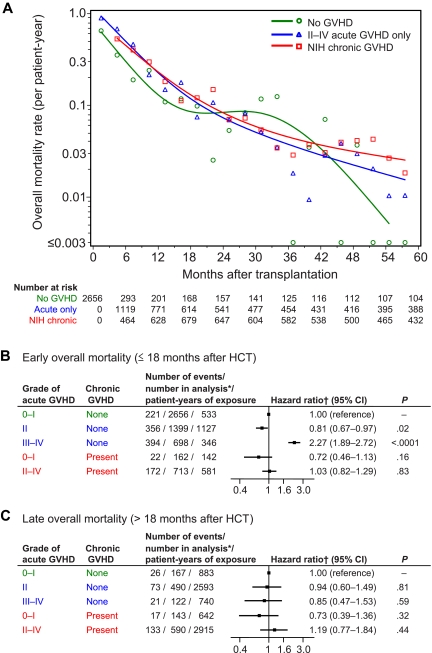
This study was conducted to elucidate the influence of immunosuppressive treatment (IST) and GVHD on risk of recurrent malignancy after allogeneic hematopoietic cell transplantation (HCT). The study cohort included 2656 patients who received allogeneic HCT after high-intensity conditioning regimens for treatment of hematologic malignancies. Rates and hazard ratios of relapse and mortality were analyzed according to GVHD and IST as time-varying covariates. Adjusted Cox analyses showed that acute and chronic GVHD were both associated with statistically similar reductions in risk of relapse beyond 18 months after HCT but not during the first 18 months. In patients with GVHD, resolution of GVHD followed by withdrawal of IST was not associated with a subsequent increase in risk of relapse. In patients without GVHD, withdrawal of IST was associated with a reduced risk of relapse during the first 18 months, but the risk of subsequent relapse remained considerably higher than in patients with GVHD. In summary, the association of GVHD with risk of relapse changes over time after HCT. In patients without GVHD, early withdrawal of IST might help to prevent relapse during the first 18 months, but other interventions would be needed to prevent relapse at later time points.
Figures


Comment in
-
Hematology: Preventing relapse.Nat Rev Clin Oncol. 2011 Jun 28;8(8):448. doi: 10.1038/nrclinonc.2011.99. Nat Rev Clin Oncol. 2011. PMID: 21709697 No abstract available.
References
-
- Appelbaum FR. Haematopoietic cell transplantation as immunotherapy. Nature. 2001;411(6835):385–389. - PubMed
-
- Socie G, Stone JV, Wingard JR, et al. Long-term survival and late deaths after allogeneic bone marrow transplantation. Late Effects Working Committee of the International Bone Marrow Transplant Registry. N Engl J Med. 1999;341(1):14–21. - PubMed
-
- Miller JS, Warren EH, van den Brink MR, et al. NCI First International Workshop on the Biology, Prevention, and Treatment of Relapse After Allogeneic Hematopoietic Stem Cell Transplantation: report from the Committee on the Biology Underlying Recurrence of Malignant Disease Following Allogeneic HSCT: graft-versus-tumor/leukemia reaction. Biol Blood Marrow Transplant. 2010;16(5):565–586. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
