

Review
doi: 10.1172/JCI45680.
Epub 2011 Jun 1.
Dynamics of insulin secretion and the clinical implications for obesity and diabetes
Affiliations
- PMID: 21633180
- PMCID: PMC3104758
- DOI: 10.1172/JCI45680
Item in Clipboard
Review
Dynamics of insulin secretion and the clinical implications for obesity and diabetes
J Clin Invest.
2011 Jun.
Abstract
Insulin secretion is a highly dynamic process regulated by various factors including nutrients, hormones, and neuronal inputs. The dynamics of insulin secretion can be studied at different levels: the single β cell, pancreatic islet, whole pancreas, and the intact organism. Studies have begun to analyze cellular and molecular mechanisms underlying dynamics of insulin secretion. This review focuses on our current understanding of the dynamics of insulin secretion in vitro and in vivo and discusses their clinical relevance.
Figures
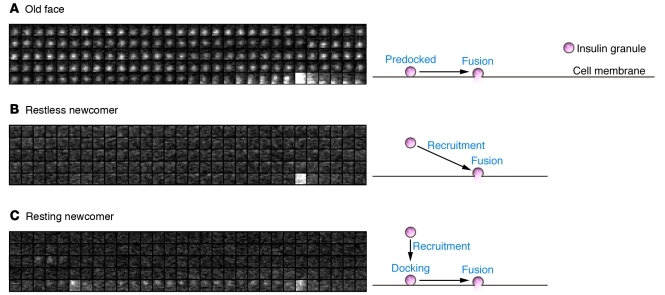
(A) Old face. Predocked granules are fused to the membrane by stimulation. (B) Restless newcomer. Granules are newly recruited and immediately fused to the plasma membrane by stimulation. (C) Resting newcomer. Granules are newly recruited, docked, and fused to the plasma membrane by stimulation. Sequential images (1 μm × 1 μm) acquired every 300 ms indicate insulin granule dynamics. Flash indicates fusion events of insulin granules. Reproduced from Proceedings of the National Academy of Sciences of the United States of America (25).
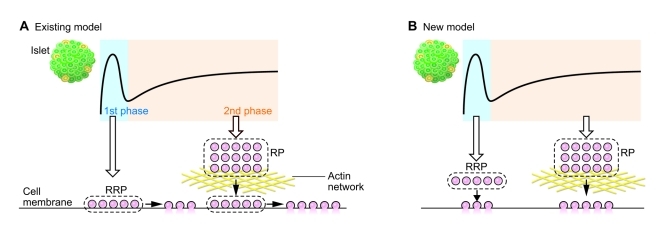
(A) In the existing model of GSIS, the first phase of insulin secretion results from a RRP composed of docked insulin granules (old face); the second phase of secretion results from a RP composed of granules located farther away (resting newcomer) that are newly recruited upon stimulation, docked, and fused to the plasma membrane. (B) In the new model, both phases consist of insulin granules that are recruited upon stimulation and immediately fused to the plasma membrane (restless newcomer). A RRP responsible for the first phase is located more than 50 nm from the plasma membrane, yet is immediately releasable. The second phase of insulin secretion involves exocytosis of insulin granules from a RP associated with the cortical actin network regulated by glucose-evoked signals in a mechanism yet to be elucidated.
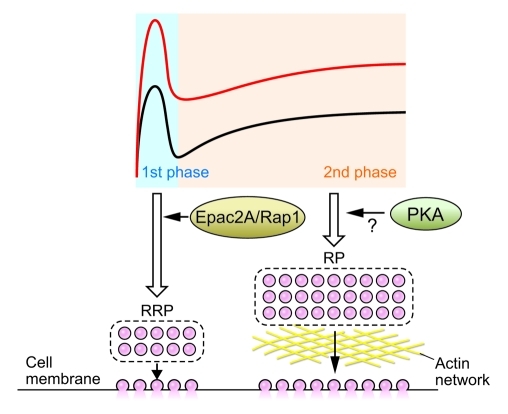
Activation of cAMP signaling enhances both the first and the second phases of GSIS. Epac2A/Rap1 signaling increases the size of a RRP near the plasma membrane. Whether Epac2A/Rap1 quantitatively or functionally increases the size is not known. The mechanism of potentiation of the second phase of GSIS by cAMP is still unclear, but PKA may be involved in regulating the size of the RP. The black line indicates dynamics of insulin secretion by glucose stimulation, whereas the red line indicates potentiation of GSIS by cAMP signaling.
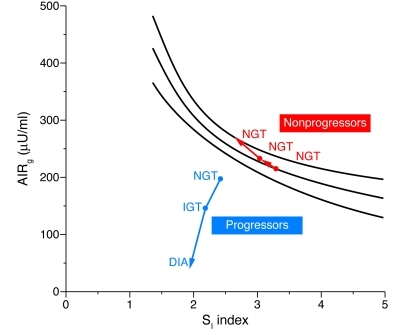
Lines represent the prediction line and the lower and upper limits of the 95% confidence interval of the regression between AIRg and SI index, as derived from a reference population of Pima Indians with NGT. Adapted from Journal of Clinical Investigation (82).
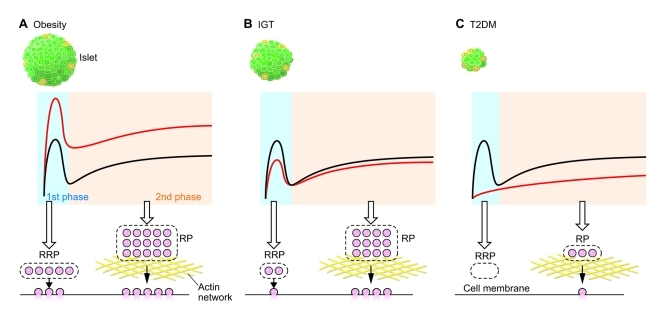
(A) In obesity, the function of individual β cells appears to be normal and both phases of GSIS are enhanced primarily due to an increase in β cell mass. (B) In IGT, the first phase is slightly impaired because of a decrease in the size of the RRP and/or partial defect in the exocytotic process of the granules in this pool, and the second phase is only moderately reduced. (C) In T2DM, the first phase is absent because of a complete loss of the RRP and/or a complete defect in the exocytotic process. The second phase is also reduced, probably due to the decreased RP and/or disturbance of cortical actin network in T2DM. Black lines indicate dynamics of insulin secretion in normal state, whereas red lines indicate insulin secretion in disease.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
