

Review
doi: 10.1016/j.jaci.2011.04.051.
Epub 2011 Jun 2.
Lung imaging in asthmatic patients: the picture is clearer
Affiliations
- PMID: 21636118
- PMCID: PMC3187916
- DOI: 10.1016/j.jaci.2011.04.051
Item in Clipboard
Review
Lung imaging in asthmatic patients: the picture is clearer
J Allergy Clin Immunol.
2011 Sep.
Abstract
Imaging of the lungs in patients with asthma has evolved dramatically over the last decade with sophisticated techniques, such as computed tomography, magnetic resonance imaging, positron emission tomography, and single photon emission computed tomography. New insights into current and future modalities for imaging in asthmatic patients and their application are discussed to potentially shed a clearer picture of the underlying pathophysiology of asthma, especially severe asthma, and the proposed clinical utility of imaging in patients with this common disease.
Copyright © 2011 American Academy of Allergy, Asthma & Immunology. Published by Mosby, Inc. All rights reserved.
Figures
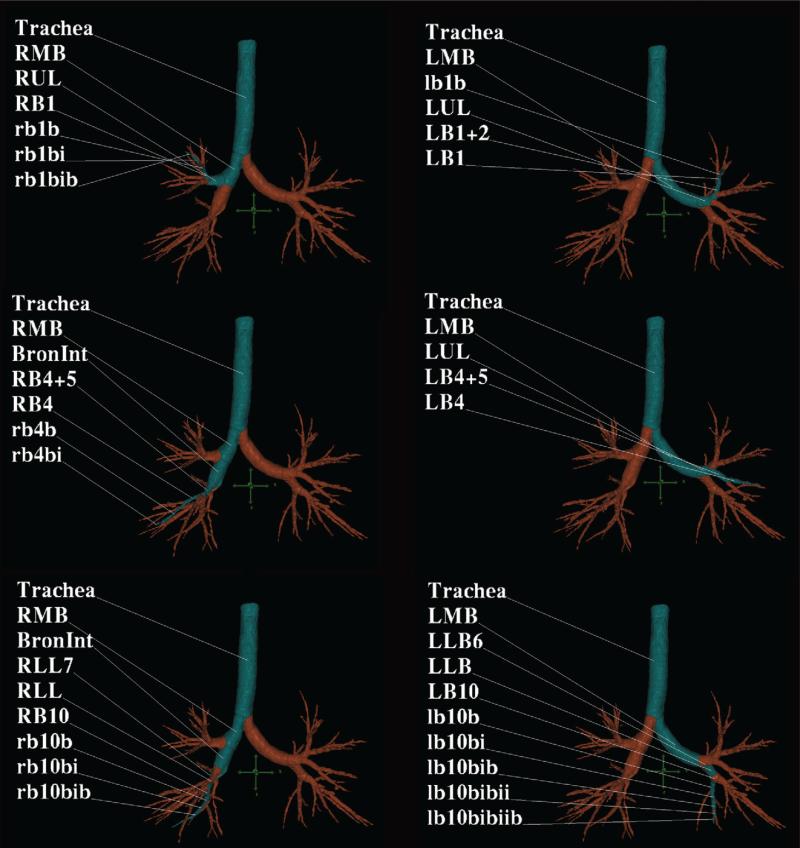
MDCT analysis was performed using the Pulmonary Workstation software (VIDA) and a screen capture of the cross-sectional MDCT image is demonstrated across three segmental pathways (in blue) in the right and left lung.
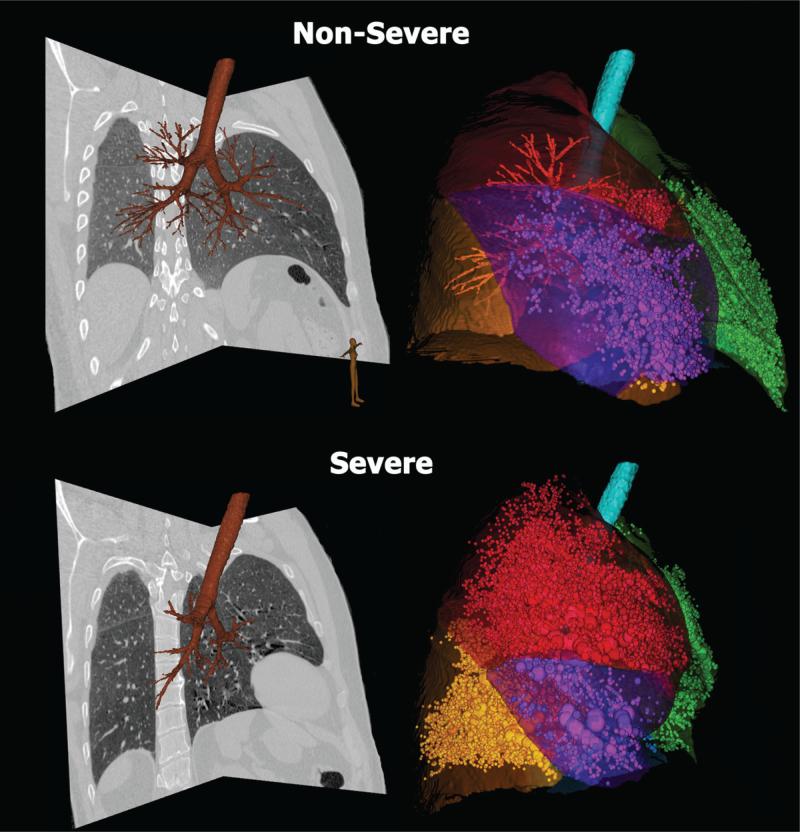
Quantitative CT allows accurate assessment of air trapping in asthma: non-severe (upper row) and severe asthma (lower row). Trapped air defined as voxels within the lung field falling below -856 HU are demonstrated by sphericals proportional to area of air trapping (volume rendered view) in the right panels. Each lobe is color-coded. Corresponding CT sagittal views are shown in the left panels. For non-severe asthmatic (upper row) the percent air trapping values (below –856 HU) are: RUL 3%, RML 17%, RLL 0.5% and LUL 6%, LLL 8%. For severe asthmatic (lower row) the percent air trapping (below –856 HU) is: RUL 28%, RML 60%, RLL 29% and LUL 25%, LLL 27%.
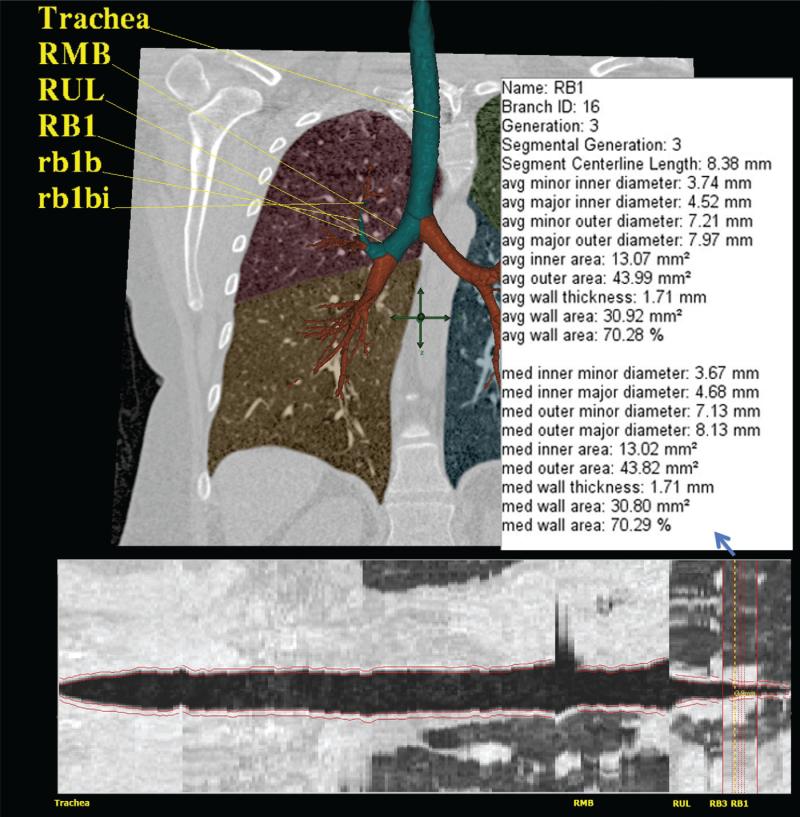
Quantitative rendering of airway tree in 3D with RB1 segmental pathway highlighted with numerical quantitative airway dimensions (upper image), and in cross-section with airway boundaries outlined in red (lower image).
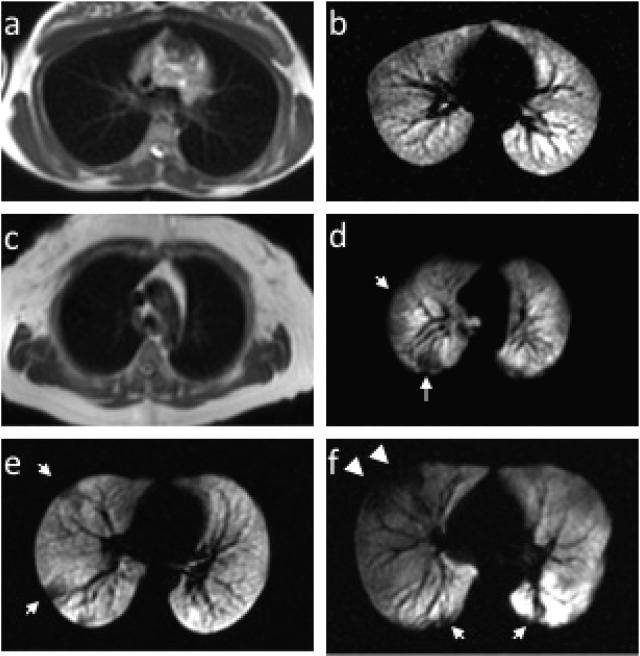
Examples of conventional proton MR images paired with corresponding slices from HP He MR images in a healthy normal subject without ventilation defects (a and b) and a healthy normal subject with ventilation defects (c and d, arrows). HP He MR images in a patient with mild-moderate persistent asthma (e) and severe asthma (f). Note the greater central extent of the defects more typical of severe asthma (f, arrowheads).
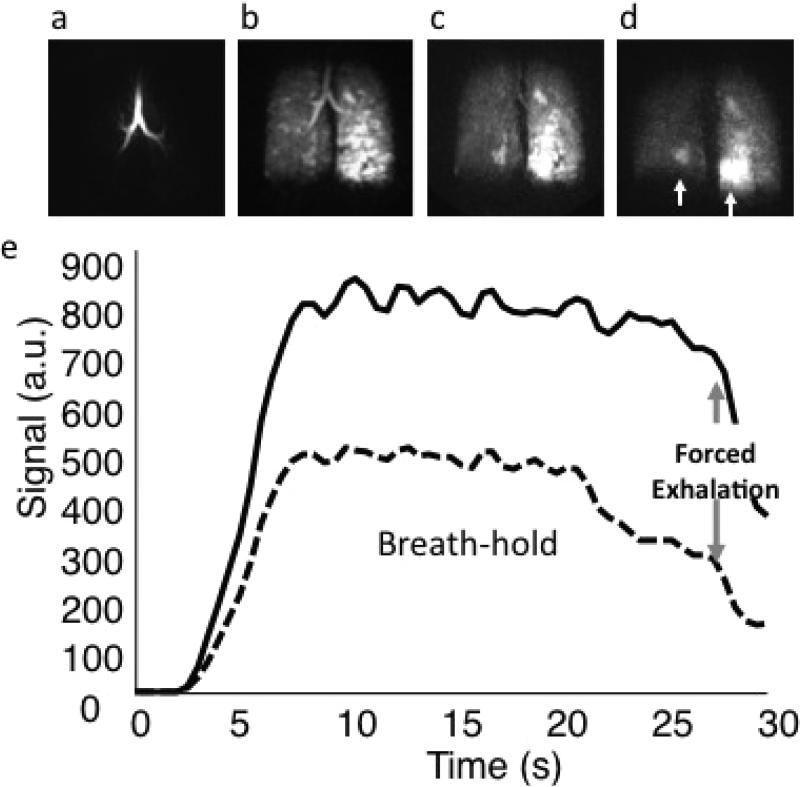
Three dimensional dynamic HP He MRI showing gas wash-in (a), breath-hold (b), and forced expiration (c and d) at a 0.5 second frame rate for a patient with moderate persistent asthma demonstrating hetereogeneous gas distribution (b) with gas trapping in the lower right and, most prominently, in the lower left lung (c and d, arrows). (e) Kinetics of wash-in and wash-out derived from regions of interest in the right upper lobe (dotted) and left upper lobe (solid) can be used to quantify regional spirometry.
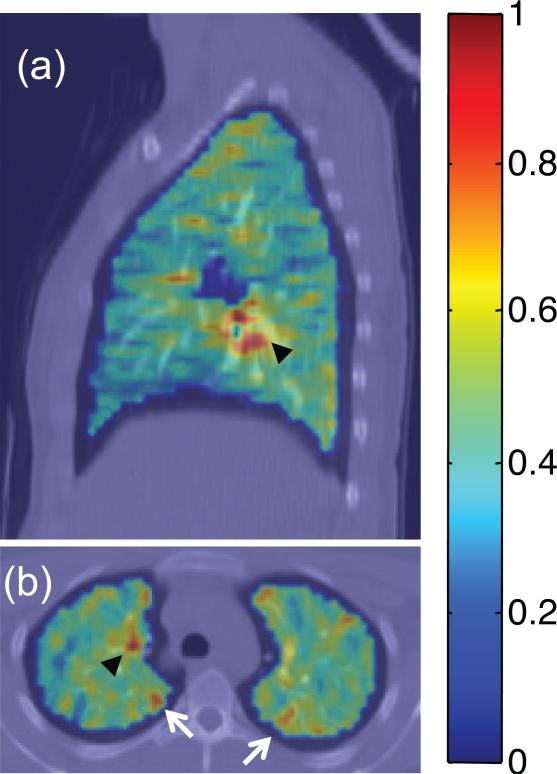
Fluorodeoxyglucose (FDG) PET/CT images depicting standardized uptake value (SUV) parametric maps overlain on CT images for a subject with mild persistent asthma during a respiratory tract infection. Areas of uptake on both (a) sagittal and (b) axial slices indicate mediastinal lymph node inflammation (black arrowheads), and selected peripheral areas of localized airway inflammation (white arrows in b).
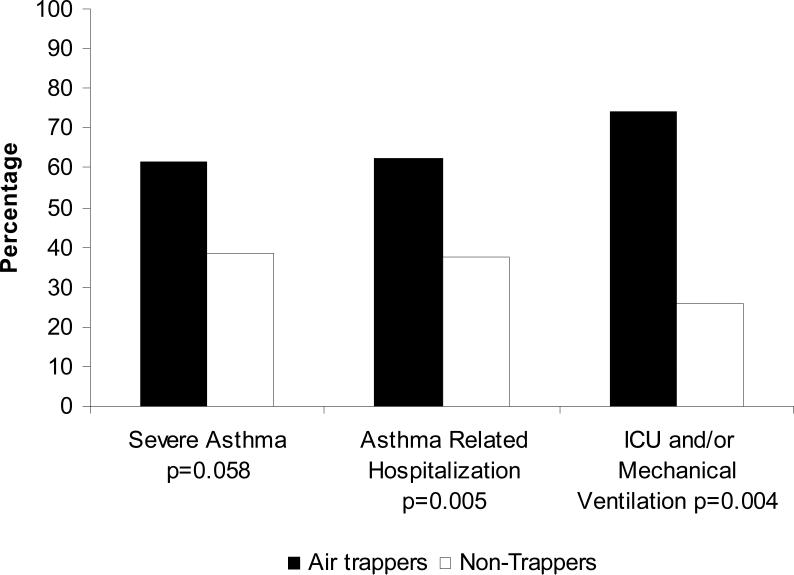
The presence of air trapping is associated with severe asthma and severe exacerbations of asthma (Reproduced with permission from Ref.).
References
-
- Benayoun L, Druilhe A, Dombret M-C, Aubier M, Pretolani M. Airway structural alterations selectively associated with severe asthma. Am J Respir Crit Care Med. 2003;167:1360–8. - PubMed
-
- Boulet L, Belanger M, Carrier G. Airway responsiveness and bronchial-wall thickness in asthma with or without fixed airflow obstruction. Am J Respir Crit Care Med. 1995;152:865–71. - PubMed
-
- Paganin F, Seneterre E, Chanez P, Daures J, Bruel J, Michel F, et al. Computed tomography of the lungs in asthma: Influence of disease severity and etiology. Am J Respir Crit Care Med. 1996;153:110–04. - PubMed
-
- Pontana F, Faivre J, Remy-Jardin M, Flohr T, Schmidt B, Tacelli N, et al. Lung perfusion with dual-energy multidetector-row CT (MDCT): feasibility for the evaluation of acute pulmonary embolism in 117 consecutive patients. J Thorac Imaging. 2008;25:100–11. - PubMed
Publication types
MeSH terms
Grants and funding
- HL69174/HL/NHLBI NIH HHS/United States
- R01 HL069116/HL/NHLBI NIH HHS/United States
- HL-69155/HL/NHLBI NIH HHS/United States
- HL69349/HL/NHLBI NIH HHS/United States
- U10 HL109250/HL/NHLBI NIH HHS/United States
- R01 HL069130/HL/NHLBI NIH HHS/United States
- HL69130/HL/NHLBI NIH HHS/United States
- R01 HL064368/HL/NHLBI NIH HHS/United States
- R01 HL069167/HL/NHLBI NIH HHS/United States
- R01 HL091762/HL/NHLBI NIH HHS/United States
- R01 HL069155/HL/NHLBI NIH HHS/United States
- HL69170/HL/NHLBI NIH HHS/United States
- HL69149/HL/NHLBI NIH HHS/United States
- HL69116/HL/NHLBI NIH HHS/United States
- R01 HL069174/HL/NHLBI NIH HHS/United States
- R01 HL069149/HL/NHLBI NIH HHS/United States
- R01 HL069170/HL/NHLBI NIH HHS/United States
- R01 HL069349/HL/NHLBI NIH HHS/United States
- UL1 RR024992/RR/NCRR NIH HHS/United States
- HL69167/HL/NHLBI NIH HHS/United States
- HL64368/HL/NHLBI NIH HHS/United States
- U10 HL109164/HL/NHLBI NIH HHS/United States
- UL1 TR000448/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
